2018 Technical Guidelines
STATE OF CONNECTICUT
TECHNICAL GUIDELINES
Health Care Response
To Victims of Sexual Assault
In accordance with Connecticut General Statutes Section 19a-112a
Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations
2017
Follow this link to download a printable version of this document (PDF Format; Size 3.8MB, PDF Format - Adobe Acrobat Reader Required).
Follow this link to download Acrobat Reader at no charge.
COMMISSION MEMBERS
CHAIRPERSON
Maureen Platt|
State’s Attorney, Judicial District of Waterbury
Designee of Chief State’s Attorney Kevin T. Kane
STATUTORY MEMBERS
Linda J. Cimino
Office of Victim Services
Connecticut Judicial Branch
Laura Cordes
Connecticut Alliance to End Sexual Violence
Marielle Daniels
The Connecticut Hospital Association
Chief James Kenny
Connecticut Police Chiefs Association
Candida Fusco MSN, RN, SANE - A
Connecticut Nurses Association
Peter Jacoby, MD, FACEP
Connecticut College of Emergency Physicians
John M. Leventhal, MD Pediatrician
Yale University School of Medicine
Patti LaMonica, MSN, RN SANE
Connecticut Emergency Nurses Association
Michelle Noehren
Connecticut Commission on Women, Children and Seniors
Sergeant Brian L. Narkewicz
Connecticut State Police
Monica Polzella
Department of Children and Families
Joy Reho
Division of Scientific Services
Department of Emergency Services and Public Protection
INTRODUCTION
History
In 1988, the Connecticut General Assembly passed Public Act 88-210, An Act Concerning Collection of Evidence in Sex Offense Crimes. The law created a multi-disciplinary Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations under the authority of the Department of Public Health, and directed it to select a standardized assault evidence collection kit and recommend a hospital protocol for sexual assault evidence collection.
In 1993, Public Act 93-340, An Act Concerning Sexual Assault Investigations, provided for the appointment of additional Commission members and transferred administrative responsibility for the Commission activities to the Division of Criminal Justice. The new Commission designed a sexual assault evidence collection program for use throughout the State of Connecticut. This program included a customized kit, to replace the standard kit selected by the 1988 Commission, and standardized forms for use by all health care facilities. The Commission also developed the State of Connecticut Technical Guidelines for Health Care Response to Victims of Sexual Assault (hereinafter referred to as Technical Guidelines), to replace the Hospital Protocol for Victims of Sexual Assault, created by the 1988 Commission. Additionally, the Commission established a uniform video training program and procedures for the payment of the evidence collection portion of sexual assault examinations.
The State of Connecticut Technical Guidelines for Health Care Response to Victims of Sexual Assault was released in 2010 and revised in 2013. In 2015, a standing subcommittee of the Commission was formed to annually review the Technical Guidelines and make recommendations to the full Commission for revision.
In acknowledgment that some sexual assaults are drug facilitated, the Commission has created a separate kit and conducted training for law enforcement investigators and health care providers.
Purpose
It is the goal of the Connecticut General Assembly and this Commission that, to the extent possible, sexual assault examinations be standardized throughout the state. To accomplish that goal, it is necessary that health care personnel who encounter or treat sexual assault victims have knowledge of what constitutes a proper and sensitive response: best practices in medical treatment, evidence collection, and follow-up services. The Technical Guidelines establish a standardized model for health care response to victims of sexual assault and the collection of sexual assault evidence.
A law enforcement agency submits the kit, including a copy of the medical report, to DESPP - Division of Scientific Services.
The Technical Guidelines do not purport to establish a standard for the medical care and treatment of sexual assault victims. All documentation generated under the Technical Guidelines shall become part of the patient’s medical record.
Pursuant to the authority granted to this Commission in Public Acts 88-210 and 93-340, the requirements of sexual assault evidence shall be set forth in the Regulations of Connecticut State Agencies.
Nothing in the Technical Guidelines is intended to create a basis in court for evidentiary standards or exclusionary motions regarding documentation or evidence. Failure to adhere to the Technical Guidelines is not intended to limit the admissibility of any documentation or evidence in a court of law or any other legal proceeding.
Acknowledgements
The Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations thanks all those who have contributed their time and expertise to this work and acknowledges that their dedication and commitment have been instrumental to the completion and revision of these Technical Guidelines.
Thank you to Diane Carberry, Margo George, Elaine Pagliaro, and Sherry Watson for their tireless efforts with the initial version of the Technical Guidelines.
Thank you also to the Evidence Commission Subcommittee that worked to review and revise the 2013 edition of the Guidelines: Linda J. Cimino, Laura Cordes, Denise Covington, Marielle Daniels, Anna Doroghazi, Candida Fusco, Patti LaMonica, Michelle Noehren, and Joy Reho, with special thanks to Anna Doroghazi and Michelle Noehren for editing this version of the Technical Guidelines.
And it is with genuine appreciation that the Commission thanks the work groups and members of the Revision of the Technical Guidelines Subcommittee who have contributed so generously of their time, work, and expertise to provide the 2017 version of the Technical Guidelines:
Subcommittee Chair: Denise Covington
Advocacy Work Group: Laura Cordes (Commission), Elise Delacruz
Forensic Lab Work Group: Cheryl Carreiro (Commission appointed), Kevin MacMillan, Karen Lamy, Dr. Michael Rickenbach, Mark Anderson, Robert DeLuca, Joy Reho (Commission), Dr. Guy Vallaro
Health Care Work Group: Candida Fusco (Commission), Kristin Loranger, Carol Michalak
Law Enforcement Work Group: James Kenny (Commission), Robin Montgomery, Marc Montminy
Legal Work Group: Anne Mahoney (Commission appointed), Bonnie Bentley, Brenda Hans, Elizabeth Leaming, Michele Lukban
Office of Victim Services Work Group: Linda J. Cimino (Commission), Anna Fidyk, Rachel McKnight
Pediatric and Adolescent Work Group: John Leventhal (Commission), Kirsten Bechtel, Audrey Courtney, Nina Livingston
Reviewers: Linda J. Cimino, (Commission), Marielle Daniels (Commission), Michelle Noehren (Commission), Jenna LoGiudice, Jennifer Cox
ORDERING INFORMATION: SEXUAL ASSAULT KITS
There are 2 types of evidence collection kits used in health care facilities:
(1) CT100B Sexual Assault Evidence Collection Kit
(2) CT400A Toxicology Screen Evidence Collection Kit
TO ORDER:
- Call (860) 263-2767
-
Leave a message with the following information:
- Your name (in case additional information is required)
- Telephone number where you can be reached
- Name of health care facility
- Mailing address of health care facility
- Quantity of each item requested
Note: CT100B Sexual Assault Evidence Collection Kits are used more frequently than CT 400A Toxicology Screen Evidence Collection Kits. Each Kit contains blood collection tubes with expiration dates. Facility stock may be used so long as the preservatives in the tubes are identical to those listed on the tubes from the Kits. Orders should be commensurate with usage.
I. CONSIDERATIONS
Sexual Assault Forensic Examiners (SAFEs)
A Sexual Assault Forensic Examiner (SAFE) is a health care provider who has fulfilled specific requirements, didactic and clinical, which enables them to perform knowledgeable and skilled medical-forensic examinations and to ensure the integrity, preservation, and documentation of forensic evidence.
-
The criteria set by the International Association of Forensic Nurses (IAFN) and the Department of Justice (DOJ) for becoming a SAFE includes current licensure, a minimum of 2 years of clinical practice, successful completion of a SAFE course which includes a minimum of 40 continuing education contact hours of classroom instruction, and “sufficient supervised clinical practice until determined competent” (Department of Justice [DOJ] National Protocol, 2013).
-
A Sexual Assault Forensic Examiner is a broad term that may include physicians as well as nurses. A Sexual Assault Nurse Examiner (SANE) is also a SAFE, but as the description is limited to nurses, the term SAFE is used so as to be inclusive of other health care providers.
-
In Connecticut, the role and responsibilities of the Sexual Assault Forensic Examiner are established by statute [Connecticut General Statutes (CGS) §19a-112(g)].
-
Some states have an advisory board which sets clinical and education requirements, as well as renewal requirements of the SAFE designation, upon expiration, usually every 3 years. Connecticut currently does not have such a board or continuing education requirements.
-
The Gail Burns-Smith SAFE Program, a Judicial Branch, Office of Victim Services program, currently responds to 8 acute care hospitals and the University of Connecticut, Storrs Campus. The SAFE Program offers a SAFE Training Program, inclusive of both didactic and clinical. Certificates awarded to those who complete the training have a three year expiration date and are renewed automatically by those who are in the SAFE Program in good standing.
-
Patients who present as victims of sexual assault at any Connecticut acute care facility may have a medical-forensic exam and evidence collection conducted at that hospital, in accordance with the Technical Guidelines, even if a SAFE is not available.
Barcodes - CT100B Sexual Assault Evidence Collection Kits
Rationale and Use:
For questions about CT100B Sexual Assault Evidence Collection Kit tracking, barcodes, or software, please email dss.saktracking@ct.gov.
Tracking all CT100B Sexual Assault Evidence Collection Kits within the state, coupled with recently enacted legislation requiring law enforcement agencies to submit all Kits to the Division of Scientific Services within 10 days, will eliminate the important public safety issue of unsubmitted Kits in the state of Connecticut.
In order to track all CT100B Sexual Assault Evidence Collection Kits within the state, the manufacturer has placed a unique barcode on the side of each Kit in addition to a sticker with the lot number/expiration date, as shown in Figure 1 below.
Figure 1: Showing barcode location on side of the Kit, located in top corner
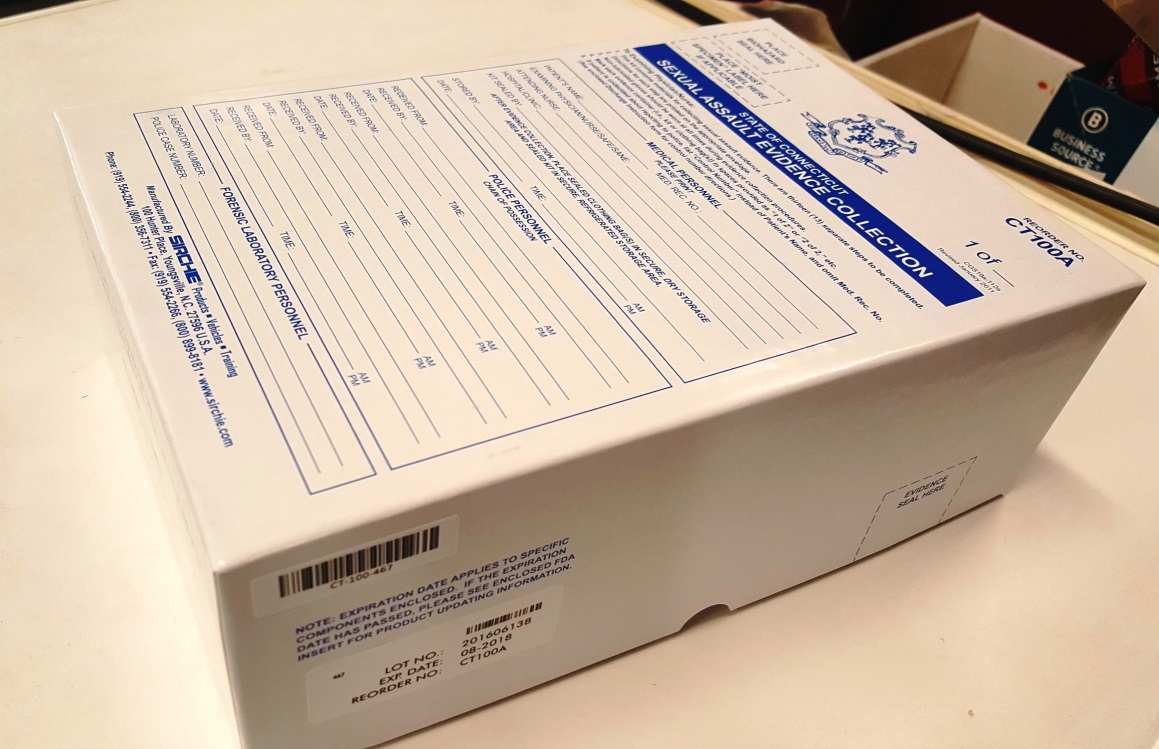
The barcode has the following sequences, either CT-###-### or CT-######, as shown in Figures 2 and 3. This six-digit number is unique and represents only 1 CT100B Sexual Assault Evidence Collection Kit. Software that allows tracking of the CT100B Sexual Assault Evidence Collection Kits was also recently installed.
Figure 2: Showing barcode with code CT-###-###

Figure 3: Showing barcode with code CT-######

-
If a CT100B Sexual Assault Evidence Collection Kit is going to be used for anything other than a sexual assault examination (training, demonstration, opened but not used, etc.) please email dss.saktracking@ct.gov with the barcode number, the facility name, and the reason for using the kit in another manner (training, demonstration, opened but not used, etc.).
-
If a CT100B Sexual Assault Evidence Collection Kit will be going to an out of state jurisdiction for testing, please email dss.saktracking@ct.gov with the barcode number, the name of the health care facility, and the state to which the Kit will be transferred.
This will ensure that all CT100B Sexual Assault Evidence Collection Kits are tracked.
Timeline for Evidence Collection
-
CT100B: Evidence should be collected up to 120 hours (5 days) from time of assault.
-
This time frame has been shown to have the most potential for the collection of semen. Evidence collected outside this time frame adds to the trauma of the patient without added benefit.
-
CT400A: Blood should be collected within 48 hours (2 days) of the suspected drugging incident. Urine should be collected within 120 hours (5 days) of the suspected drugging incident.
Consent for Medical/Forensic Examination and Evidence Collection
-
Consent is required for a medical/forensic exam and evidence collection [CGS §19a-112a (d)].
No one should be forced against his/her will to undergo a sexual assault evidence collection examination.
The CT100B Sexual Assault Evidence Collection Kit
-
Prior to opening the Kit, briefly describe the evidence collection and examination process with the patient. Ensure that communication is being provided in the patient’s preferred language.
-
The patient must have the capacity (be oriented to person, place, time, and able to participate in care and make their wishes known) in order to provide consent.
-
Consult your facility’s policies and procedures for obtaining consent for incapacitated patients, persons with cognitive disability, proxy-decision care takers (including but not limited to any specific policies for a patient that is conserved or has an appointed healthcare representative, and/or is severely injured or incoherent due to drugs or alcohol intoxication).
-
The Kit contains a written consent form: Authorization for the Sexual Assault Medical Exam and Release of Payment Information. After reviewing the consent form, have the patient or patient’s representative sign the form.
-
The white original of the signed, completed authorization form should be placed in the patient’s medical record.
-
As the medical-forensic examination is performed, explain each step with the patient before taking action on that step - the patient can decline any part of the exam. Document the reason the step was declined on the step envelope.
-
Report to Law Enforcement:
-
There is no requirement that law enforcement be notified in order for evidence to be collected. Only notify law enforcement with patient consent (verbal will suffice). Please note the patient is able to change their mind at any time.
-
Consult your facility’s policies and procedures for mandatory reports to law enforcement that may still apply.
-
If the patient is undecided about whether to report to law enforcement, explain the importance of prompt evidence collection, and that the evidence can be held for 5 years to give them time to decide.
-
Explain that the evidence can be submitted anonymously and held up to 5 years.
-
Explain also that during the 5-year period the evidence will be identified by a control number, not by their name.
-
-
Please note that law enforcement should not be included among those allowed in the examining room during the exam and evidence collection process.
-
-
A Sexual Assault Crisis (SAC) Advocate:
-
A sexual assault advocate should be allowed to explain their role directly to the patient prior to services so that the patient can make an informed decision as to whether or not they desire advocacy services.
-
A sexual assault advocate should be allowed to accompany the patient throughout the process with patient consent (verbal will suffice).
-
See Appendix F for further information on obtaining a SAC Advocate.
-
The CT400A Toxicology Screen Evidence Collection
-
Testing for the presence of drugs and/or alcohol in the system of a sexual assault patient is not suggested or required unless medically indicated or indicated by the patient’s case history. If the decision is made to collect samples for toxicology testing:
-
Review the Consent for Toxicology Screen form contained within the CT400A Kit with the patient.
-
Have the patient or patient’s representative sign the consent form.
-
The white original of the signed and completed consent form should be placed in the patient’s medical record.
-
Minors: Considerations for Obtaining Consent:
-
Consent for the medical-forensic exam and evidence collection of a minor (anyone under the age of 18) should be obtained from the parent or guardian (verbal will suffice).
-
Any known or suspected child sexual abuse/assault should be reported to law enforcement and to the Department of Children and Families (DCF) [CGS §17a-101(a-e)] - consult your facility’s policies and procedures on mandatory reporting.
-
In the rare event that a minor presents with a parent/guardian who refuses to consent to the examination of the child, consult your facility's policies and procedures regarding refusals of consent by parents/guardian.
-
If it is determined that the child is in danger from her/his surroundings and requires immediate attention, the attending physician can take the child into custody at the hospital for 96 hours [CGS §17a- 101(f)] – this allows for health care personnel to provide diagnosis and treatment, and child protective and law enforcement agencies to investigate any sexual abuse/assault while protecting the child from further immediate danger).
-
Law Enforcement
-
When the patient wants to report to law enforcement at the time of the exam:
-
Law enforcement needs to obtain basic facts from the patient in order to identify the assailant and to locate primary and secondary crime scenes. The primary being where the actual assault occurred and a secondary being where items of evidence may have been left by the patient (i.e. bedroom clothes hamper if they changed clothing).
-
The quicker law enforcement can identify the crime scene and secure it, the higher the likelihood useable evidence may be collected to support the patient's allegations.
-
-
When the patient does not want to report to law enforcement at the time of the exam:
-
The role of law enforcement in the case where a patient does not want to report the incident is more of a guardian of the evidence. If an anonymous Kit is completed, then the law enforcement agency within the health care facility’s jurisdiction will be responsible for collecting the Kit from the facility and transporting it back to the department.
-
-
Purpose and scope of patient’s statements made to law enforcement:
-
Statements made by a patient to a law enforcement officer can be admitted as evidence by that officer. These statements can corroborate the patient’s allegations. Law enforcement needs to identify who the patient may have confided in prior to coming to the health care facility. This person can testify regarding statements/allegations made by the patient and are admissible as an exception to the hearsay evidence rule. These statements may also be made to the examiner during the medical-forensic exam.
-
-
Informational needs of law enforcement:
-
Identification of suspect or description of suspect.
-
Location (specific) where the assault occurred.
-
Identification of witnesses.
-
Permission from the patient to retrieve clothing and other evidence from their residence.
-
In depth follow up interviews will be conducted in the days following the initial report. In most instances, basic facts of the case are all that is needed at this point to facilitate actions of law enforcement.
-
Law Enforcement presence in the exam room:
-
Law enforcement has no need to be present during the forensic exam. All items of evidentiary value are collected by the forensic-medical examiner and are sealed in evidence bags per the Kit instructions.
-
Law enforcement can be allowed access post-exam if the patient is capable and consents to further questioning. Otherwise law enforcement will take possession of the completed evidence Kits.
-
-
How law enforcement handles anonymous Kits (Kits not reported at the time of the exam):
-
The protocol for the processing of anonymous Kits is the same both within and outside the State of Connecticut.
-
The anonymous Kits are received from the medical-forensic examiner after the chain of custody form is completed.
-
The anonymous Kits are transported to the police department where the medical facility is located, called the department of jurisdiction.
-
The department of jurisdiction will ensure that the anonymous Kit is transported to the Forensic Lab within 10 days of receipt. According to Public Act 15-207, the anonymous Kit will be retained by the Forensic Lab for 5 years.
-
Victims of sexual assault have up to 5 years to report from date of assault.
-
Maintaining chain of custody from healthcare:
-
Of primary importance for a criminal prosecution for sexual assault is maintaining the chain of custody. This is particularly true of the sexual assault evidence Kit.
-
In the legal sense the chain of custody is the electronic or written documentation of transfer of the collected evidence from the party who collected it, to the party responsible for storage, to the party responsible for scientific testing and processing, and ultimately for presentment in court as evidence.
-
Each time the evidence changes hands it is signed for by the receiving party to document that the evidence is the same as collected and it remains substantially the same upon presentment in court.
-
The chain begins when the medical-forensic examiner collects the evidence and then seals it within the Kit. The examiner signs the chain of custody form, which in turn is signed by the officer receiving the Kit. This establishes the legal reliability of the evidence upon presentment in court.
-
Failure to follow the chain of custody allows for the legal challenge of the reliability of the evidence at trial.
-
-
Identify what information law enforcement may need from health care providers within the boundaries of patient privacy laws:
-
Interviews of patients who are reporting at the time of the exam are critical to law enforcement in order to establish a base line or their version of events.
-
The patient may identify their assailant or witnesses to the act; they may also identify where the assault occurred or identify articles of evidence that may be lost or destroyed by the suspect.
-
Visual evidence gathered by the medical-forensic examiner will also provide valuable evidence to support the information provided by the patient. Articles of torn clothing and defensive type wounds or injury all support the claims that force was used.
-
This information is valuable for the criminal investigator who may be tasked with the initial interviews of a potential suspect to dispel claims that the patient willingly participated in the act.
-
Law enforcement does not need information about unrelated medical history which may be obtained during the medical exam.
-
-
II. THE MEDICAL-FORENSIC EXAM PROCESS
Initial Contact and Triage
-
Sexual assault patients are trauma patients and should be triaged as priority patients regardless of whether physical injuries are evident.
-
Assess for safety concerns upon arrival and identification of the sexual assault patient.
-
Assess for injuries and provide medical care and treatment prior to collecting evidence. Clothing should be placed in paper, rather than plastic, bags.
-
Provide a private area in which the patient can await both intake and treatment.
-
Assess age, communication ability and health condition. Modify response accordingly.
-
If translation services or a sign language interpreter is needed, follow health care facility policy in accordance with federal requirements, and record on CT100B forms.
-
If a patient must go to the bathroom, explain that semen or other evidence may be present in pubic, genital, and rectal areas, and not to wash or wipe away those secretions until after the examination.
-
Health care facilities participating in the Gail Burns-Smith Sexual Assault Forensic Examiners Program (SAFE Program) may activate an on-call SAFE according to protocol.
- The SAFE will call the local sexual assault crisis program to activate an advocate.
-
For non-participating health care facilities, follow the Technical Guidelines, in addition to your facility’s protocol, for care of the sexual assault patient.
Advocacy – The Connecticut Alliance to End Sexual Violence
- There are 9 sexual assault crisis programs in Connecticut. Each center provides the same core services:
-
24-hour toll free confidential hotline.
-
Certified sexual assault victim advocates.
-
Medical, police, and court accompaniment and advocacy.
-
Support groups.
-
Spanish-speaking and male advocates, upon request.
-
Information and referral .
-
Community education.
-
Short term supportive counseling.
-
-
To contact the program that covers your area, please consult the program map in Appendix F.
-
You can also call the hotline at 1-888-999-5545 from your facility’s landline and you’ll be connected to the local sexual assault crisis program.
-
Health care facilities should call the advocate as soon as the patient arrives.
-
When calling an advocate please be sure to tell them:
-
Patient’s age
-
First name of the patient or nurse they should ask for
-
If a Spanish-speaking advocate is needed
-
-
Once the advocate arrives, with the patient’s verbal consent, the advocate should be allowed into the room to introduce themselves to the patient and explain their role.
-
Sexual assault victim advocates will support the patient throughout their time in the health care facility.
-
This includes, but is not limited to:
-
Providing immediate crisis counseling and advocacy.
-
Informing the patient of their rights and available resources.
-
-
-
Unless the patient requests otherwise, the advocate will stay with them throughout the entirety of the exam, and their stay in the hospital.
-
With the patient’s consent, the advocate will also sit with them while they are giving their statement to law enforcement.
-
When notifying the advocate, let the advocate know roughly what size clothing to bring for the patient to wear upon discharge.
-
Spanish-speaking victim advocates are available. However, they cannot act as the interpreter. Please follow facility policies.
-
If the patient does not want the advocate to stay, the advocate will leave contact and general program information with the patient.
-
Advocates are not there to help with the evidence collection, but to support the patient, and to ensure the patient is informed about their options.
Sensitivity and Cultural Concerns
-
Treat the patient with dignity and respect. Introduce yourself, acknowledge the trauma they have experienced, and explain the exam process. Give the patient time to respond. Do not rush.
-
Keep in mind that the medical-forensic exam and evidence collection is likely to be the first significant physical contact that a patient will have following an assault.
-
Ask for permission before touching the patient in any way. Allow the patient to regain control and to make their own decisions.
-
Avoid asking “why” questions; instead use open-ended questions such as, “what, how, where, tell me…, describe…” Avoid judgmental responses and facial expressions.
-
Be aware and tolerant of the patient’s language skills and communication barriers, which may be worsened by crisis.
-
Coordinate with staff to avoid asking the patient to repeat their account of the assault numerous times (e.g., triage, nurse, physician, social worker).
-
Keeping the patient’s needs in mind, exercise discretion and sensitivity when discussing patient’s case with other personnel.
-
Be aware that discussing sexual assault or sexual terms may be associated with shame and embarrassment in some cultures, and that in some cultures the loss of virginity is devastating.
-
Recognize that beliefs about women, men, sexuality, sexual orientation, race, culture, religion, and sexual assault may be very different among patients – never assume anything.
Supplies for the Medical-Forensic Exam and Evidence Collection
-
A private examining room, with attached bathroom, is best for the sexual assault patient. A gynecologic stretcher should be used for the exam.
-
A stocked sexual assault cart stored in the designated examining room will eliminate the need to gather essential examining equipment after the patient has arrived.
-
Needed items:
-
Non-powdered gloves
-
Masks
-
Disposable gowns
-
Disposable bonnets
-
Disinfectant wipes
-
Sealed CT100B and CT400A Kits
-
Sterile saline solution
-
Several cotton-tipped swab packets
-
Speculum-assorted sizes
-
Alternate light source or Woods Fluorescent Lamp
-
Tape
-
Pen and pencil
-
Swab dryer or Styrofoam/paper cups
-
Large brown paper bags (grocery type)
-
Portable bedside table
-
-
Recommended Items:
-
Sterile gauze packets
-
Stapler and staples
-
Locked refrigerator designated as an evidence storage unit
-
-
If a swab dryer is not available, have a stable table/counter space available for air drying specimens away from people in the room.
Preparation for the Medical-Forensic Exam and Evidence Collection
-
DNA - Touch DNA:
-
Also called “contact DNA”. This is DNA from skin cells left behind from touching or coming into contact with an object/person.
-
The amount of DNA left behind depends on multiple factors, such as: length of time in contact, type of substrate, whether the individual is a “shedder,” and amount of pressure or friction applied.
-
-
DNA - Testing:
-
DNA testing has increased in sensitivity greatly over recent years. DNA profiles can be detected from as few as 1-2 human cells.
-
It is imperative that extraneous DNA contamination be prevented from DNA samples that will be examined in a forensic laboratory.
-
-
To prevent cross-contamination and ensure a clean environment when collecting evidence:
-
Gloves should be worn and changed frequently: between steps and between evidentiary locations, as well as after touching any potentially contaminated objects (pens, stethoscopes, etc.).
-
Disposable gown or covering for clothing. This keeps cells that are on daily worn clothing from contaminating samples.
-
Face masks should be worn by all within 3 feet of the evidence. The mask should be worn over both mouth and nose.
-
Bonnets or hairnets should be worn.
-
Use sanitation procedures at the health care facility including disinfectant wipes and/or cleaning solutions. Equipment used, such as pens, pencils, and, cameras should also be cleaned.
-
Presence of Others in the Exam Room
-
Generally, only the examining and attending health care providers should be in the room during the examination. With patient consent, a sexual assault advocate may also be present.
-
If the patient requests the presence of a close friend or family member, this request should be honored after discussing possible legal ramifications of being present during the history, exam, and collection of evidence.
-
Advocates have privileged communications; they cannot be compelled to testify without patient consent. All others present during the forensic exam may be subpoenaed.
-
There is no medical or legal reason for a law enforcement officer (male or female) to be present during the forensic history and exam.
Documentation
General Points:
-
Use objective neutral wording. Do not use “alleged” or “claims,” instead write “Patient states.” Also, write “declined” rather than “refused.” In health care, the patient is a patient, not a victim nor a survivor.
-
Describe objectively what is observable with the senses. Avoid vague terms such as “poor” or “good.”
-
Do not use abbreviations.
-
Read back the patient’s responses in order to ensure accuracy.
-
Review all CT100B and CT400A forms at the end of the exam to ensure they are completely filled out and signed. Distribute white, yellow and pink copies as noted on the bottom of the pages.
-
The original of the CT100B and CT400A forms (white pages) should be retained and scanned – front and back – by the health care facility as part of the medical record
The Medical-Forensic History
General Points:
-
The history is not the same as an investigative interview. It is a history of the assault, as relayed by the patient, as part of the medical-forensic exam, and will become a part of the medical record.
-
The history is intended to guide the exam, evidence collection, and forensic lab analysis of the findings. The Division of Scientific Services uses the history to “triage” their examination of the Kit.
-
The history takes place after medical care for acute injuries, but before evidence collection.
-
Presence of family members, friends or other persons in the room, aside from the advocate, may influence, or be perceived as influencing, patient history. They should be aware they may be subpoenaed.
-
These other individuals should only be present if patients (including minors) choose to have them present. They should not answer questions for the patient, interrupt the patient or make facial expressions in response to answers so as to influence the account of the assault.
-
Taking the history:
-
Sit at eye level with the patient, at the head of the bed. It is not necessary to wear gloves or mask during the history, which can be perceived as a barrier.
-
Explain to the patient that the account of the assault needs to be taken verbatim. In the history, identify the patient as the historian (e.g., “Patient states.…”). Use quotes.
-
Writing firmly and legibly, record the account of the assault as it is relayed by the patient.
-
Do not ask leading questions. Do not paraphrase or summarize.
-
It may be necessary to ask the patient to speak slower, take a break for you to catch up, and/or read-back to the patient what is written in order to ensure accuracy.
-
Photography
-
Specific written informed consent should be obtained according to facility policies prior to photography.
-
Photographs should be taken by a knowledgeable photographer, preferably by law enforcement with appropriate equipment. Findings should be photographed without a scale, and then with a scale for reference.
-
Colposcopy photographs and other images of the genital area should not be taken unless the patient provides written consent.
-
Transfer or Storage of images should be in accordance with facility policy.
-
Photographs should not be placed inside the CT100B kit.
-
Exam and Evidence Collection
It is important to understand the evidentiary purpose of the exam. According to the National Protocol, “The findings in the exam and collected evidence provide information to help reconstruct the details about the events in question in an objective and scientific manner.” Patients should understand the exam is not about routine medical care.
Note: On September 19, 2016, the Commission voted to omit the head and pubic hair pull steps in accordance with a request from the Division of Scientific Services as hair analysis is no longer conducted.
Steps for CT100B Evidence Collection
Step 1: Known Blood Sample – Rationale and Use: Evidence samples from sexual assaults may contain DNA mixtures of more than 1 individual. It is important to know the DNA profile of the patient so that evidentiary DNA profiles can be interpreted as accurately as possible.
-
A sample of blood is superior over a known buccal or known oral swab because these samples may be contaminated due to an oral sexual assault or oral contact.
-
If the CT400A Toxicology Screen Evidence Collection Kit is to be collected, blood samples from this kit should be collected prior to the CT 100B blood sample. Blood needed for hospital tests should be drawn in conjunction with, but after, forensic tubes are collected.
-
Order of Draw:
-
CT 400A gray top tubes
-
CT 100B purple top tube
-
Hospital labs
-
-
Expired tubes from the Kits may be replaced with the same from facility stock, so long as tube preservatives are identical to those listed on the blood collection tubes from the Kits. Document replacement on step envelope.
-
Procedure:
-
Wear gloves, mask, disposable gown, and hairnet/bonnet.
-
Ask permission to draw blood.
-
Draw blood using order of draw above.
-
Place patient label, date and initial, on tube(s).
-
Replace purple top blood tube in enclosed bubble pack bag, using adhesive strip to seal.
-
Once known blood sample is collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
If blood is drawn for the CT400A, return tubes to the cardboard holder in the CT400A Kit.
-
Step 2: Oral Swabs and Smear – Rationale and Use: This sample may be tested for semen in the patient's oral cavity. Blood may be tested to show force. The swabs may be forwarded for DNA analysis.
-
When indicated by patient history, samples may be collected from around the exterior mouth and lip area. The sample should not be collected as an oral specimen, but as a dried secretion specimen for Step 6.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab mouth.
-
Assemble swab boxes.
-
The collector’s initials and date should be on the outside of the slide container.
-
Ensure that the frosted side of the slide is face up.
-
Using enclosed pencil, write the following on the frosted area of the slide: patient’s initials, date, “oral.”
-
Use the first set of 2 unmoistened swabs to simultaneously swab between the buccal and the gingival line around the oral cavity.
-
Turn swabs between thumb and forefinger while swabbing. This ensures that all swab surfaces are exposed to sample.
-
-
Use this first set of swabs to make a smear: Roll one swab across the slide in a 360° roll. Repeat this with the second swab directly underneath the first roll.
-
Dry swabs and place into the swab box labeled “Oral Smear.”
-
Repeat swabbing of oral cavity with second set of 2 unmoistened swabs.
-
Dry swabs and place in the second swab box labeled “Oral Swabs.”
-
Once swabs and smear are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
Step 3: Clothing – Rationale and Use: Analysis is conducted for debris, fluids, and other evidence. All testing of evidence taken from clothing, including cuttings and swabbing will be conducted by the DESPP-DSS (Department of Emergency Services and Public Protection, Division of Scientific Services).
-
Do not cut through any holes, rips or tears in clothing when removing from patient. Ask and document if damage to clothing was due to the assault.
-
Leave obvious debris intact on clothing, and package as found.
-
Document if clothing has been changed since the assault. If original clothing worn during assault is at a different location, document location. Relay information to law enforcement so clothing can be collected and submitted to the Forensic Lab.
-
Collect underwear worn/removed during the assault. Collect underwear changed into after the assault. Document each bag clearly.
-
Use additional clean paper bags, as needed. Never use plastic bags.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Place clean hospital sheet on floor. Place unfolded paper sheet from kit on top of hospital sheet.
-
Have patient stand on paper sheet and disrobe. Protect modesty.
-
Ask permission for each item of clothing collected.
-
Collect each clothing item as it is removed.
-
Place each item separately in the appropriate bag. Use extra bags as needed.
-
Separate visible stains and moist areas with clean paper towels to avoid contamination.
-
If items are wet or damp, air-dry as much as possible before packaging.
-
Let law enforcement know when transferring evidence to them that items are damp so they can continue the drying process upon transfer.
-
Refold paper sheet so that any debris is contained. Place patient label, date and initials on it before placing it into large outer clothing bag.
-
Once all clothing evidence is collected, seal (make sure bags are sealed end to end) and label bags and envelopes in accordance with instructions on Evidence Integrity.
-
Step 4: Debris – Rationale and Use: Debris and trace materials noted during the forensic examination may be used to corroborate the case history.
-
Debris includes (but is not limited to) the following: soil, grass, leaves, weeds, and bark (outdoors); clothing or carpet fibers, human, dog or cat hair, paint or glass chips (indoors).
-
Debris is collected from the patient’s body; not from the patient’s clothing.
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to examine patient and collect debris.
-
Collect debris observed on patient’s body. Look carefully for hairs and small trace items.
-
If the debris is too large for the envelope provided, place in a clean paper bag, secure in accordance with instructions on Evidence Integrity. Label with identification and chain of custody information.
-
Document location of debris on envelope with anatomical location where debris was found on the patient’s body. Use words and arrows to show location.
-
Once all debris evidence is collected, seal and label envelope in accordance with instructions on Evidence Integrity.
Step 5: Fingernail Swabbings and Clippings – Rationale and Use: Document whether the patient recalls scratching the face, body or clothing of the suspect (for Touch DNA). Based on this information, or if it was a violent assault, these samples may be examined for blood and tissue like material to show force. These samples may be forwarded for DNA analysis.
-
Do not clip acrylic nails. Use lightly moistened swabs (sterile saline) to swab under acrylic nails. Document this on the envelope in the space.
-
If nails are too short to clip, lightly moisten swabs with sterile saline to swab the tip area of the nails, avoiding the fingertips. Document this on the envelope in the space provided.
-
Procedure:
-
This step contains 1 step envelope, 2 specimen envelopes labeled “right hand” and “left hand”, 1 swab packet, 2 swab boxes labeled “right hand” and “left hand,” and 1 pair of fingernail clippers.
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab and clip fingernails.
-
Open swab packet and remove both swabs. Moisten swabs lightly with sterile saline.
-
Using 1 swab per hand, lightly swab underneath the fingernails, avoiding fingertips. Dry swabs.
-
Carefully clip the nails over the appropriate specimen envelope for each hand.
-
Seal clippers inside the step envelope, and the swab for each hand inside the appropriate swab box.
-
Complete the label.
-
Once swabs and clippings are collected, seal and label envelope in accordance with instruction on Evidence Integrity.
-
Step 6: Dried Secretion Specimen – Rationale and Use: This sample may be tested for body fluids from the patient's body. These samples may be forwarded for DNA analysis.
-
Important: If the sample is of a “touch” nature and testing for a body fluid is not indicated, see Step 7 for the collection of “Touch” DNA. Unnecessary testing for a body fluid would be a waste of sample and could negatively impact the ability to get a DNA result.
-
Important: Note the location and potential body fluid, as indicated by history, on the diagram. It allows laboratory personnel to conserve sample and save time.
-
Use a light touch when swabbing. A heavy touch will result in a concentration of the patient’s DNA, rather than the assailant’s.
-
An alternate light source with filter or Woods Fluorescent Lamp in a darkened room may help locate dried secretions. Collect a sample regardless of the absence of fluorescence as indicated by history.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab indicated areas.
-
Pre-assemble swab box. Lightly moisten set of 2 swabs with sterile saline (1 or 2 drops each).
-
To Swab:
-
Start at the outside of the indicated area.
-
Swab lightly in a circular pattern, turning swabs between thumb and forefinger. This ensures that all swab surfaces are exposed to the sample.
-
Use separate swab sets for each indicated location. Use facility stock as needed.
-
Dry swabs and place into swab box. Place any extra swabs into their packets. Document location where each swab set was taken as indicated by history or alternate light source findings.
-
Once swabs are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
-
Step 7: Touch DNA – Rationale and Use: Also called “contact DNA”. This is DNA from skin cells left behind from touching or coming into contact with an object/person. Touch DNA may be obtained from the skin when strangulation has occurred, or the patient was forcefully grabbed. Do NOT swab clothing for “Touch” DNA.
-
The amount of DNA left behind depends on multiple factors, such as: length of time in contact, type of substrate, whether the individual is a “shedder,” and amount of pressure or friction applied.
-
DNA testing has increased in sensitivity greatly over recent years. DNA profiles can be detected from as few as 1-2 human cells.
-
Use a light touch when swabbing. A heavy touch will result in a concentration of the patient’s DNA, rather than the assailant’s.
-
Procedure:
-
Change gloves, mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab indicated areas of touch DNA.
-
Pre-assemble swab box. Lightly moisten set of 2 swabs with sterile saline (1 or 2 drops each).
-
To Swab:
-
Start at the outside of the indicated area.
-
Swab lightly in a circular pattern, turning swabs between thumb and forefinger. This ensures that all swab surfaces are exposed to the sample.
-
Use separate swab sets for each indicated location. Use hospital stock as needed.
-
Dry swabs and place into swab box. Place any extra swabs into their packets. Document location where each swab set was taken as indicated by history.
-
Once swabs are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
-
Step 8: Pubic Hair Combings – Rationale and Use: The purpose of this sample is to collect hairs foreign to the patient (e.g., transfer from suspect). This sample may be forwarded for DNA analysis.
-
Patient may have shaven pubic region. Comb for foreign pubic hair even if shaven.
-
If hair is matted with a substance, with permission, cut matted area with sterile scissors and place in Step 12 specimen envelope. Document cut specimen on front of envelope.
-
If patient declines cutting of matted substance, swab area with swabs obtained from hospital stock, lightly moistened with sterile saline. Dry swabs and return to swab packet. Label swab packet with contents. Place in Step 8 envelope.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to comb pubic region.
-
Place unfolded specimen envelope under patient’s buttocks.
-
Comb through pubic region, retaining any loose hairs within envelope.
-
Re-fold envelope, enclosing any loose hairs and comb.
-
Once public hair combings are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
Step 9: Genital Swabs – Rationale and Use: This sample may be tested for semen or saliva from the patient’s genital area and forwarded for DNA analysis. This sample may be tested for blood to show force.
-
If no vaginal swabs (Step 10) are collected for female patients, a minimum of 2 additional genital swabs should be collected.
-
Note: If indicated, samples from the inner thighs should be collected as Touch DNA (Step 7) or as a Dried Secretion Specimen (Step 6), depending on case history.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab genital area.
-
Assemble swab boxes. Open 2 swab packets and remove swabs. Moisten swabs lightly with 1 or 2 drops of sterile saline prior to specimen collection.
-
Females: Using first set of swabs, lightly swab in the following order: across labia minora, fossa navicularis (where the labia minora meet posteriorly), labia majora, and groin (mucosal to non-mucosal areas). See diagram on step envelope. Repeat with second set of swabs.
-
Males: Use first set of swabs as follows: scrotum, groin, shaft of penis, and glans. Repeat with second set of swabs.
-
Dry swabs and place into appropriate swab boxes.
-
Place swab boxes inside step envelope. Label and seal the envelope and return it to Kit.
-
Once swabs are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
Step 10: Vaginal Swabs and Smear – Rationale and Use: This sample may be tested for semen or saliva in the patient’s vaginal cavity and the swabs forwarded for DNA analysis. This sample may be tested for blood to show force.
-
If testing for sexually transmitted infections (STIs), specimens should be performed immediately following forensic specimen collection.
-
Vaginal swabs should be collected from the posterior fornix, below the cervix.
-
An external genital exam should be conducted prior to specimen collection. The face of a clock, superimposed over the genital area, should be used to describe location of injuries (e.g., abrasion noted from 5 to 7 o’clock).
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab vaginal cavity.
-
Assemble swab boxes.
-
The collector’s initials and date should be on the outside of the slide container.
-
§ Ensure that the frosted side of the slide is face up.
-
Using enclosed pencil, write the following on the frosted area of the slide: patient’s initials, date, “vaginal.”
-
-
Use warm water to moisten speculum. Do not use lubricant. Once speculum is in place, inspect the internal vaginal cavity for injuries, using a clock face to describe the location of any noted injuries.
-
To collect specimens: use the first set of 2 swabs to swab the posterior fornix.
-
Turn swabs between thumb and forefinger while swabbing. This ensures that all swab surfaces are exposed to sample.
-
Use this first set of swabs to make a smear: Roll 1 swab across the slide in a 360° roll. Repeat this with the second swab directly underneath the first roll.
-
Dry swabs and place into the swab box labeled “Vaginal Smear.”
-
Repeat swabbing of posterior fornix with second set of 2 swabs. Dry swabs and place in the second swab box labeled “Vaginal Swabs.”
-
Once swabs and smear are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
Step 11: Anal Swabs and Smear – Rationale and Use: This sample may be tested for semen or saliva in the patient’s anal cavity and the swabs forwarded for DNA analysis. This sample may be tested for blood to show force.
-
An external anal exam should be conducted prior to specimen collection. Anal folds should be gently separated to examine for injury.
-
Swabs should be lightly moistened with 1 or 2 drops of sterile saline.
-
Swabs should be collected from inside the anal cavity to the depth of the cotton tip of the swab.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to swab anal cavity.
-
Assemble swab boxes.
-
The collector’s initials and date should be on the outside of the slide container.
-
Ensure that the frosted side of the slide is face up.
-
Using enclosed pencil, write the following on the frosted area of the slide: patient’s initials, date, and “Anal.”
-
-
-
To collect specimens: use the first set of 2 swabs to swab anal cavity to the depth of the cotton tip of the swab.
-
Turn swabs between thumb and forefinger while swabbing. This ensures that all swab surfaces are exposed to sample.
-
Use this first set of swabs to make a smear: Roll 1 swab across the slide in a 360° roll. Repeat this with the second swab directly underneath the first roll.
-
Dry swabs and place into the swab box labeled “Anal Smear.”
-
Repeat swabbing of anal cavity with second set of 2 swabs. Dry swabs and place this set in the second swab box labeled “Anal Swabs.”
-
Once swabs and smear are collected, seal and label envelope in accordance with instructions on Evidence Integrity.
Step 12: Other Physical Evidence – Rationale and Use: Other physical evidence may include condoms, tampons, sanitary pads, tissue, or other debris inside vaginal or anal cavities. These items may be examined for body fluids and/or used to corroborate case history.
-
Do not swab the surfaces of other physical evidence; any sample collection will be performed at the Forensic Lab.
-
For moist specimens, use the yellow “Moist Evidence” sticker located inside the envelope. Place in the appropriate place on the front of the kit.
-
Do not place moist specimens directly into paper envelope. Contents may leak through and contaminate other specimens.
-
Procedure:
-
Change gloves, wear mask, disposable gown, and hairnet/bonnet.
-
Ask permission to collect other physical evidence.
-
Place moist specimens inside plastic bag(s) and seal.
-
Once other evidence is collected, seal and label envelope in accordance with instructions on Evidence Integrity.
-
Steps for CT400A Toxicology Screen Evidence Collection
-
Routine toxicology testing is not recommended. However, in any of the following situations, the collection of a urine and/or blood sample may be indicated:
-
The patient’s medical condition appears to warrant toxicology screening (e.g., drowsiness, fatigue, light-headedness, dizziness, physiologic instability, memory loss, impaired motor skills, severe intoxication).
-
The patient or accompanying person states that the patient was or may have been drugged.
-
The patient suspects drug involvement because of a lack of recollection of the assault.
-
Blood (10 mL in each tube) should be collected in conjunction with the CT100B, with the toxicology gray top tubes being first in the order of draw. Urine (60 mL) should also be obtained when doing the CT400A Toxicology Screen Evidence Collection Kit.
-
Urine will not be tested for GHB (gamma-hydroxybutyric acid) when the urine collection time is more than 12 hours beyond the suspected drugging incident.
-
Blood will not be tested for GHB (gamma-hydroxybutyric acid) when blood collection time is more than 8 hours beyond the suspected drugging incident.
-
Neither blood nor urine will be tested for ethanol when sample collection time is more than 24 hours beyond the suspected drugging incident.
-
Urine testing will not be conducted more than 120 hours (5 days) beyond the suspected drugging incident.
-
Blood testing will not be conducted more than 48 hours (2 days) beyond the suspected drugging incident.
-
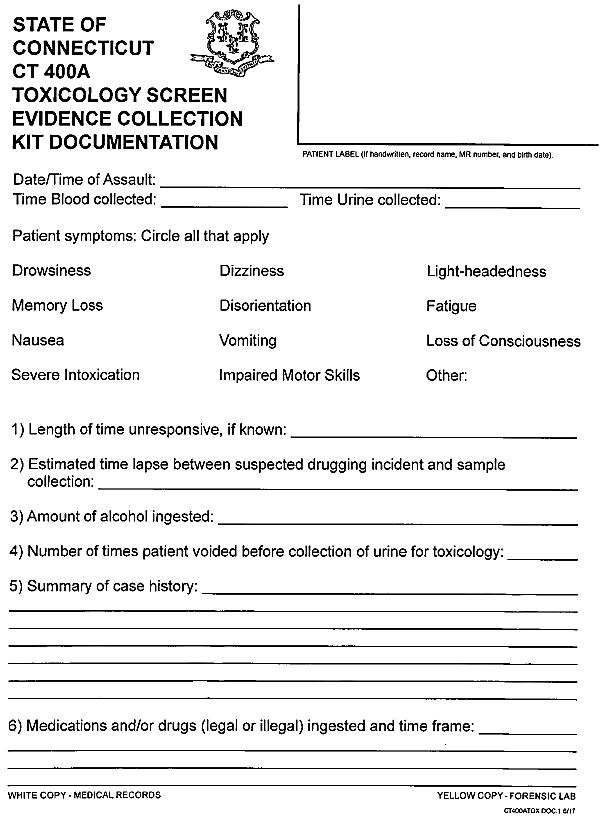
CT400A Documentation
-
Required information includes, but is not limited to:
-
Date/time of assault.
-
Date/time of blood and urine collection.
-
Patient symptoms.
-
Length of time unresponsive.
-
Time lapse between suspected drugging incident and sample collection.
-
Amount of alcohol ingested.
-
Number of times patient voided before collection of urine for toxicology.
-
Case history – provides needed information to the toxicologist and allows for efficient testing.
-
Any pre-hospital (legal or illegal) or in-hospital medications that have been taken since the incident.
-
Blood
-
To be collected within 48 hours of suspected drugging incident.
-
Blood specimens will be examined for drugs/metabolites which have been identified within the associated urine specimen.
-
Collect 10 mL of blood in each gray top tube, following directions provided in kit. Use only gray top tubes containing sodium fluoride and/or potassium oxalate (provided in kit). Facility stock may be used so long as blood collection tube preservatives are identical to those listed on the blood collection tubes in the CT 400A kit.
-
Once blood sample is collected, seal and label accordance with instructions on Evidence Integrity.
-
Urine
-
To be collected within 120 hours (5 days) of the suspected drugging incident.
-
Urine is considered “the best” specimen for most drug-facilitated sexual assault cases.
-
Collect 60 mL of urine, following directions, in the cup provided in the kit.
-
30 mL of urine is needed for testing, but limited testing can be performed with volumes less than 30 mL of urine.
-
Once urine is collected, seal and label in accordance with instructions on Evidence Integrity.
Storage
-
Blood and urine must be refrigerated after collection. While samples can be frozen, care must be taken that sample containers do not break or crack. All primary specimen containers should be stored within a secondary container (e.g., zip-lockable plastic bag) to prevent loss or contamination due to leakage.
Sexually Transmitted Infections (STIs) Evaluation and Care
The following is intended to serve as a guide for the care and treatment of the sexual assault patient.
The medical care and treatment of sexual assault patients should be consistent with current professional guidelines and accepted medical practice. The following is taken from the Centers for Disease Control (CDC) at: https://www.cdc.gov/std/tg2015/sexual-assault.htm
-
Baseline testing at the time of the initial exam does not typically have forensic value if patients are sexually active and a STI could have been acquired prior to the assault. However, baseline serum testing for HIV, Hepatitis B, and Syphilis should be considered on a case by case basis.
-
If testing, specimens for STI testing should be performed immediately following forensic specimen collection.
-
Patients who prefer prophylaxis generally do not require baseline testing.
-
Assess for allergies prior to providing medication.
-
Consider an antiemetic with the medication.
-
The CDC offers the following empiric antimicrobial regimen for chlamydia, gonorrhea, and trichomonas.
Recommended Regimens
-
Ceftriaxone 250 mg IM in a single dose (Gonorrhea)
PLUS -
Azithromycin 1 g orally in a single dose (Chlamydia)
PLUS -
Metronidazole 2 g orally in a single dose(Trichomoniasis)
OR -
Tinidazole 2 g orally in a single dose
-
If alcohol has been recently ingested or emergency contraception is provided, metronidazole or tinidazole can be taken at home rather than as directly observed therapy to minimize potential side effects and drug interactions.
-
Clinicians should counsel persons regarding the possible benefits and toxicities associated with these treatment regimens; gastrointestinal side effects can occur with this combination.
-
The efficacy of these regimens in preventing infections after sexual assault has not been evaluated.
Additional information on recommendations from the CDC can be found at: http://www.cdc.gov/std/tg2015/sexual-assault.htm
Non-occupational Post-exposure Prophylaxis (nPEP)
According to the CDC, HIV seroconversion has occurred in persons whose only known risk factor was sexual assault or sexual abuse, but the frequency of this occurrence likely is low.
-
In consensual sex, the per-act risk for HIV transmission from vaginal intercourse is 0.1%–0.2%, and for receptive rectal intercourse, 0.5%–3%.
-
Risk for HIV transmission from oral sex is substantially lower. Specific circumstances of an assault (e.g., bleeding, which often accompanies trauma) might increase risk for HIV transmission in cases involving vaginal, anal, or oral penetration.
-
CDC recommendations for post-exposure HIV risk assessment of adolescent and adult patients within 72 hours of sexual assault.
-
Determination of the assailant’s HIV status at the time of the assault examination is usually not possible. Therefore, health care providers should assess any available information concerning the:
-
Characteristics and HIV risk behaviors of the assailant(s) (e.g.,, being an MSM or using injection drugs);
-
Local epidemiology of HIV/AIDS;
-
When an assailant’s HIV status is unknown, determinations regarding risk for HIV transmission to the patient should be based on 1) whether vaginal or anal penetration occurred; 2) whether ejaculation occurred on mucous membranes; 3) whether multiple assailants were involved; 4) whether mucosal lesions are present in the assailant or patient; and 5) any other characteristics of the assault, patient, or assailant that might increase risk for HIV transmission.
-
-
Consult with a specialist in HIV treatment if nPEP is being considered.
-
If the patient appears to be at risk for acquiring HIV from the assault, discuss nPEP, including benefits and risks.
-
If the patient chooses to start nPEP, provide enough medication to last until the follow-up visit at 3–5 days after initial assessment and assess tolerance to medications.
-
If nPEP is started, perform CBC and serum chemistry to establish a baseline.
-
Perform an HIV antibody test at original assessment; repeat at 6 weeks, 3 months, and 6 months.
Note: Assistance with nPEP-related decisions can be obtained by calling the National Clinician’s Post Exposure Prophylaxis Hotline (PEP Line) (telephone: 888–448–4911) 9 a.m. – 9 p.m. EST, seven days a week. Website link: http://nccc.ucsf.edu/clinician-consultation/pep-post-exposure-prophylaxis/
Consultation can also be made with the hospital Infectious Disease Specialist.
Emergency Contraception (EC)
Sexual assault patients should be offered prophylaxis for pregnancy, subject to informed consent and consistent with current treatment guidelines (DOJ National Protocol, 2103).
-
A pregnancy test should be conducted (with patient consent) with all patients of childbearing age to establish the patient’s present status.
-
EC should be discussed as a treatment option. Taking EC after a sexual assault decreases a woman’s chances of becoming pregnant.
-
The FDA has approved Plan B pills to be initiated up to 72 hours, and Ella to be initiated up to 120 hours, but are most effective when taken within 12 hours of the assault.
-
Consider providing an antiemetic with EC.
-
Legislation was signed into law in October 2007 in Connecticut that establishes emergency contraception as a standard of care for acute care hospitals that provide emergency treatment to victims of sexual assault. This includes:
-
Providing each victim of sexual assault with medically and factually accurate and objective information relating to emergency contraception;
-
Informing such victim of sexual assault of the availability of emergency contraception, its use and efficacy;
-
-
Providing emergency contraception to such victim of sexual assault at the facility upon the request of such victim, except that a licensed health care facility shall not be required to provide emergency contraception to a victim of sexual assault who has been determined to be pregnant through the administration of a pregnancy test approved by the United States Food and Drug Administration; and
-
No licensed health care facility that provides emergency treatment to a victims of sexual assault shall determine such facility’s protocol for complying with the standard of care requirements on any basis other than a pregnancy test approved by the United States Food and Drug Administration.
-
Three current methods of emergency contraception (EC) include:
-
Plan B to be initiated within 72 hours after assault.
-
Ella to be initiated within 120 hours after assault.
-
Copper Intrauterine Device (IUD) to be inserted within 120 hours after the assault.
-
-
Best practice is to have patient begin EC as soon as possible.
Discharge Instructions
-
Allow a patient who so desires to brush their teeth. If clothing was collected, try to ensure that the patient does not leave the facility in hospital gown and slippers.
-
Whenever a sexual assault patient is discharged from the hospital or transferred to an inpatient department, the CT100B Discharge Instructions should be reviewed with the patient and a copy should be given to the patient, along with a copy of the consent form(s).
-
Referrals and resources should also be provided and discussed at this time.
-
Ensure that the patient understands the importance of follow-up care in 2 weeks.
-
If the patient is undecided whether to report the assault to police, place a Control Number on the front of the Kit(s) and Clothing Bag, as well as on the Discharge Instructions. See page 43 for instructions on how to create a Control Number.
Evidence Integrity – Sealing Evidence Bags
-
Inner Evidence Bags:
-
Double-fold the top of each inner bag. Staple or tape across the fold to seal. A patient sticker may also be used to seal.
-
Place a patient sticker, along with collector’s signature, date and time on the front of the bag.
-
-
Outer Clothing Bag:
-
The top of the brown clothing bag is double-folded. The bag should be taped across the entire fold of the bag, from one end to the other. The bag may be stapled prior to the placement of tape.
-
-
Initial 2 of the 4 Evidence Integrity stickers (these are fragile – handle carefully) and place a sticker around each end of the fold.
Labeling the Outside of the CT100B Kit and Clothing Bags and the CT400A Kit: Reporting and Not Reporting Control Number
-
If the case is a reported case (reported at the time of the exam):
-
The patient’s name and Medical Record number is placed on the front of the CT100B and Clothing Bag(s), and CT400A.
-
-
If the case is not a reported case (patient is undecided at the time of the exam - or states they will report later):
-
Control Number: Whenever a patient is undecided about reporting the assault to law enforcement, a control number must be placed on the outside of the Kits and Clothing Bag.
-
This control number is recorded in 4 places:
-
The outside of the CT100B Kit
-
The outside of the CT400A Kit
-
The consent form (bottom of page)
-
The discharge form from the CT100B (right side of form)
-
-
Control Number format: Name of Health Care Facility: Patient Initials: 6 Digit Kit Completion Date. Ex: Hospital Name: ABC: mm/dd/yy.
-
A colon separates the hospital name, the patient initials and the kit completion date.
-
Example: A patient named Anne Marie Smith has a kit completed at Nutmeg Hospital on July 17, 2017. The Kit Control number would be: Nutmeg Hospital:AMS:07/17/17
-
-
Testimony Considerations
-
The role of the health care provider is to provide accurate, unbiased information regarding the evaluation and treatment of the patient, including the statements made by the patient, the patient’s demeanor, any injuries observed, and the collection of evidence.
-
In addition to providing factual information, the health care provider may be called upon to provide expert testimony related to their advanced training, work experience with patients, and medical knowledge.
-
Accordingly, doctors, nurses, and paramedics are routinely called as witnesses at trial regarding the medical evaluation and treatment rendered to a person who has been sexually assaulted.
-
In the courtroom, the health care provider is a neutral unbiased professional who could be called to testify regarding the medical evaluation and treatment of the patient.
-
The relationship between State’s Attorneys and law enforcement is as follows:
-
Prosecutors rely on law enforcement officers to investigate an allegation that someone has committed a crime.
-
In many cases, law enforcement makes an arrest at the scene of a crime. The person arrested is then brought to court for a judge to determine if there is probable cause to believe that the arrested person committed the crime charged by law enforcement. The prosecutor then determines whether to proceed with the case. This is known as an on-site arrest case.
-
In other cases, law enforcement will not make an immediate on-site arrest, but instead, will conduct a thorough investigation and provide the information they have collected to the prosecutor. Law enforcement documents the information gathered in an arrest warrant affidavit. The prosecutor will then review the case and decide if there is sufficient evidence to present the case to a judge for the issuance of an arrest warrant. If so, a prosecutor will sign the arrest warrant and then provide it to a judge for review. If the judge determines that there is probable cause for an arrest, they will sign the arrest warrant authorizing an arrest of the accused person.
-
A prosecutor may decline to request an arrest warrant if they determine that the evidence collected by law enforcement is not sufficient to prove that a crime has been committed, or to prove who committed the crime.
-
The prosecutor also may order further investigation, either by law enforcement, or in unusual cases, by an investigatory grand jury. Once an arrest warrant is signed by a judge, the person named in the warrant is arrested and the case begins its way through the court system.
-
How the Medical Exception to Hearsay Rule Works
-
At trial, health care providers are permitted to testify about what a patient says to them while seeking medical treatment. This is called the medical exception to the hearsay rule.
-
“Hearsay” means a statement, other than one made by the declarant/witness while testifying at the proceeding, offered in evidence to establish the truth of the matter asserted. In other words, hearsay is generally understood as a rule to exclude witnesses testifying in court about statements made by another person outside of court.
-
The idea behind the exclusion is that if the speaker of the statement is not present in the courtroom, then the speaker cannot be cross-examined about those statements. This makes it unfair to the side/party who did not call the witness.
-
There are exceptions to this rule of excluding hearsay. One of the exceptions to the normal rule excluding out of court statements is the medical exception to the hearsay rule.
-
Connecticut state courts follow the Connecticut Code of Evidence which states the medical exception to hearsay as follows:
A statement made for the purposes of obtaining a medical diagnosis or treatment and describing medical history, past or present symptoms, pain, or sensations, or the inception or general character of the cause or external source thereof, insofar as reasonably pertinent to the medical diagnosis or treatment [is not excluded under the hearsay rule].
Connecticut Code of Evidence § 8-3 (5).
Examples:
-
In State v. Griswold, 160 Conn. App. 528, 555-558, cert. denied, 320 Conn. 907 (2015), the Connecticut Appellate Court held that a five year old sexual assault victim’s statements made in a forensic interview were admissible under the medical exception to the hearsay rule. The court concluded that “the victim’s statements were reasonably pertinent to obtaining medical diagnosis and treatment to bring them within the scope of the medical diagnosis and treatment section.”
-
In State v. Martin M., 115 Conn. App. 166, 174-176 cert. denied, 293 Conn. 908 (2009), the Connecticut Appellate Court held that a sexual assault patient’s statements made to a certified nurse practitioner were within the “chain of medical treatment” and admissible at trial under the medical exception to the hearsay rule. Moreover, the court found that the patient’s statements made nine months after the last sexual assault were still made for the purposes of ongoing medical treatment.
-
In State v. Donald M., 113 Conn. App. 63, 70-71, cert. denied, 291 Conn. 910 (2009), the Connecticut Appellate Court reaffirmed that the medical treatment exception applies to psychological as well as somatic illnesses and conditions. In other words, statements made to a psychiatrist or psychologist for purposes of diagnosis and treatment are admissible under the medical exception. State v. Wood, 208 Conn. 125, 133-134 (1988).
-
In addition, in order to be admitted under the medical treatment exception, the statements need not have been made to a physician, as long as they were “made in furtherance of medical treatment.” State v. Slater, 285 Conn. 162, 186 (2008) (nurse); State v. Cruz, 260 Conn. 1, 10 (2002) (social worker); State v. Maldonado, 13 Conn. App. 368, 372, cert. denied, 207 Conn. 808 (1988) (security guard used as translator).
The Crawford Doctrine
-
An accused person on trial has the right to confront the witnesses against him/her.
Usually confrontation occurs during cross examination of the witnesses when testifying in the courtroom. In Crawford v. Washington, 541 U.S. 36 (2004), the United States Supreme Court made clear that if a witness is not available for cross-examination, then his/her “testimonial statements” are not admissible in court. In other words, if the witness is available for cross-examination, then that person can testify about what he/she previously said. If that person is not available for cross-examination, whether that statement can be admitted in court depends upon if it is “testimonial” or “nontestimonial.”
-
“Testimonial” statements in general are considered statements whose primary purpose is to establish or prove events such that the conversation essentially is an out-of-court substitute for trial testimony. For example, statements made as a result of a formal interrogation at a police station, or affidavits made under oath are considered “testimonial.” These are all essentially statements given in anticipation of future litigation.
-
“Nontestimonial” statements are those made under circumstances objectively indicating that the primary purpose of the conversation is not for future use in court. For example, statements made during an emergency situation or statements made in response to a teacher’s questions about a child’s safety at home are considered “nontestimonial.” Additionally, Connecticut courts have held that nontestimonial statements include a patient’s statements to his/her healthcare provider. Therefore, these nontestimonial statements may be admissible at trial without the patient having to testify to them.
APPENDIX
Appendix A
Specific Populations
-
American Indian and Alaska Native
-
College Students
-
Elderly (age 60 and older)
-
Inmates
-
Lesbian, Gay, Bisexual, Transgender, Queer (LGBTQ)
-
Males
-
Military
-
Patients with Disabilities
-
Undocumented Immigrants
-
Victims of Human Trafficking
American Indian and Alaska Native
-
Recognize that Indian tribes may have their own laws and regulations, as well as their own police, prosecutors, advocates, courts, and service providers to address sexual assault.
-
Responders should be familiar with procedures for coordinating services and interventions for victims from these communities and should work with community groups to develop plans for providing exams to members of Indian tribes.
College Students
-
Due to the insular nature of campuses, many students may be worried about their confidentiality. It is important to remind them that their information will not be reported to their college or university without their consent.
-
Students may not know that having a medical forensic exam and evidence collection done at a hospital does not impact any investigation done on campus.
-
Eh campus has on-campus confidential support students can access. This support may look different depending on the campus resources.
Elderly (age 60 and older)
-
Elderly patients will likely experience humiliation, disbelief, and denial just as other patients do, but in addition, may also have an increased awareness of their own vulnerability.
-
Elderly patients should be consulted in all decisions regarding their care, unless their history indicates they have diminished mental capacity.
-
Hearing impairment and other physical conditions due to advancing age may be present. It is important not to confuse trauma with conditions sometimes associated with advanced age.
-
Health care providers should take care with positioning, particularly when conducting a genital assessment and collecting evidence.
-
Be aware that elderly patients may be victims of abuse perpetrated by their caretaker(s).
-
Medical and counseling follow-up services should be made easily accessible, otherwise, older patients may not be willing or able to seek or receive assistance.
Guidelines and forms regarding mandatory reporting requirements when the patient is age sixty or older are in Appendix E.
Incarcerated People
-
The Prison Rape Elimination Act (PREA) of 2003 gives prisoners equal rights to medical forensic exams and protects individuals from sexual assault in prison.
-
Inmates should be treated the same as any other patient who presents as a victim of sexual assault.
-
Medical information and treatment is confidential, as it is for other sexual assault patients.
Lesbian, Gay, Bisexual, Transgender, Queer (LGBTQ)
-
Do not make assumptions about a patient’s sexuality.
-
Patients may be reluctant to report or consent to the medical forensic exam and evidence collection due to societal views.
-
Ask the patient their preference of name and pronoun when referring to them, or speaking to others about them.
-
Be aware that they may use non-standard labels for body parts. Ask for clarification when needed.
-
Be mindful about possibly disclosing patient's sexuality to others that may be present.
-
LGBTQ patients should not feel compelled to disclose aspects of their identity they are uncomfortable disclosing.
-
“Know and Tell Why” before you ask an invasive question. Make sure it is necessary to do so as a health care provider. Also, make sure the patient is aware of why this information is necessary for health care providers to know.
Males
-
Male patients may be more likely to exhibit a controlled response after the assault, expressing feelings of shock, disbelief and confusion. The assault may cause the patient to question his own masculinity. Concerns regarding sexual identity may arise for homosexual, bisexual, or heterosexual males.
-
Although there may not be as many male sexual assault patients presenting to health care facilities as female patients, it is imperative that male sexual assault patients are treated with the same level of support and care as a female sexual assault patient.
-
Special care should be taken in packaging the male patient's clothing, especially underpants and pants because the patient may have experienced an ejaculation. To avoid cross contamination with the offender's semen, place clean, dry paper towels between moistened areas of the garment.
-
The lower back, thighs, and buttocks should be carefully examined for dried secretions using the Alternate Light Source or Woods Lamp.
-
The male sexual assault patient's oral cavity, glans, scrotal, and perianal area should be carefully examined for trauma/evidence and documented.
-
Male patients should be offered STI prophylaxis, including nPEP, as appropriate.
Military
-
The military offers victims the option of restricted reporting or unrestricted reporting.
-
Restricted reporting allows a sexual assault victim to confidentially disclose the details of his or her assault to specified individuals and receive medical treatment and counseling without initiating an official investigative process or command notification.
-
Benefits include treatment, advocacy, counseling, time to consider options, control of personal information, and patient decides whether to move forward in process.
-
Limitations include assailants going unpunished, loss of crime scene evidence, and inability to discuss with friends in the military.
-
Restricted reporting can be rendered null and void if the medical facility contacts law enforcement or other professionals other than advocates, chaplains, and military sexual assault response coordinators.
-
-
Unrestricted reporting is the reporting option for a victim of sexual assault to disclose that he or she is the victim of a sexual assault, without a request for confidentiality or restricted reporting,
-
Benefits include having a dedicated victim advocate, Commander action, victim-witness assistance, possible delay in collateral misconduct punishment, case management and monitoring, status reports, offender accountability, investigation, and possible prosecution or administrative actions.
-
Limitations include inability to change to restricted reporting, details and identities may become known, intrusive legal process, lengthy investigation or court proceedings, possible victim punishment for collateral misconduct, possible retaliation, if not properly protected by the Command.
-
-
Sexual assault evidence collection and documentation is retained for 5 years, with the option of retaining for 50 years at Service member’s request (OVCTTAC, Strengthening Military-Civilian Community Partnerships to Respond to Sexual Assault).
Patients with Developmental Disabilities
-
Patients with developmental disabilities may have limited cognitive ability, impaired and/or reduced mental capacity to understand questions. They may also have limited language/communication skills to state what happened. They may not understand that they have been a victim of crime.
-
Respect the patient’s wishes to have, or not have, caretakers, family members or friends present during the exam. These individuals may be accustomed to speaking on behalf of the patient, but it is essential they not influence the statements of the patient during the exam.
-
Speak directly to the patient, even when an interpreter or others are present.
-
If a patient has communication problems, use a word board, or other assistance as needed.
-
Allow additional time as necessary for explanations, evaluation, medical/forensic exam and evidence collection. Do not assume the patient needs special help. Ask permission before touching or helping.
-
Guidelines and forms regarding mandatory reporting requirements when the patient is developmentally disabled are in Appendix E.
Undocumented Immigrants
-
If the patient or someone in the patient's family is undocumented then they are unlikely to seek medical care.
-
The State of Connecticut will reimburse health care facilities for the cost of the sexual assault exam and evidence collection, regardless of immigration status.
-
Patients can receive care without Immigration and Customs Enforcement (ICE) being contacted. Victims of sexual assault may qualify for temporary immigration benefits through the Department of Homeland Security. Information may be obtained at: https://www.uscis.gov/i-918
Human Trafficking
Sexual assault is clearly a part of sex trafficking, but sexual assault is often a part of labor trafficking cases as well. Some considerations when working with potential sex and labor trafficking victims:
-
Be mindful of your language; do not use words such as “prostitute” when speaking with or about the patient.
-
In cases of sex trafficking, a patient may be branded with a tattoo of the pimp’s name.
-
Because of the grooming process, many sex trafficking victims may not openly identify as being a victim of trafficking.
-
Labor trafficking victims may fear reporting to law enforcement, especially if they are immigrants and their papers are being held by their traffickers.
-
In Connecticut, no one under the age of 18 can be arrested for prostitution. This may be beneficial information to share with patients.
If a patient is suspected of being a victim of human trafficking, call the DCF Careline immediately at 1-800-842-2288.
Appendix B
Pediatric Population
-
General Information
-
Consent for Exam and Evidence Collection
-
Counseling and Support
-
Algorithm for Care
General Information
-
The Technical Guidelines is intended as a reference for the adult and adolescent sexual assault patient. However, the information contained in this Appendix is intended to be used as a resource when a pre-pubescent child presents as a patient.
Consent for Examination and Evidence Collection
-
Under 13: Consent for evidence collection (verbal will suffice) should be obtained from the parent/guardian of every child under the age of 13 (except as described below). Consent should also be obtained from every child under the age of 13 who is capable of doing so.
-
No patient should be forced against her/his will to undergo a sexual assault examination and evidence collection.
-
In the event that the parent/guardian refuses to consent to an examination of the child, and if it is believed that the child is in danger from her/his caretakers and is in need of immediate attention, the attending physician may take the child into custody at the hospital for a period of 96 hours [CGS § 17a-101(g)]. This allows health care personnel to provide immediate assessment, diagnosis and treatment, and allows child protective and law enforcement agencies to investigate any sexual assault/abuse, and protect the child from further danger.
Counseling and Support
-
The Connecticut Alliance to End Sexual Violence (The Alliance) should be always called to ensure the presence of a support person.
-
The Alliance has advocates specially trained to provide support for cases involving children. They may be reached at 1-888-999-5545.
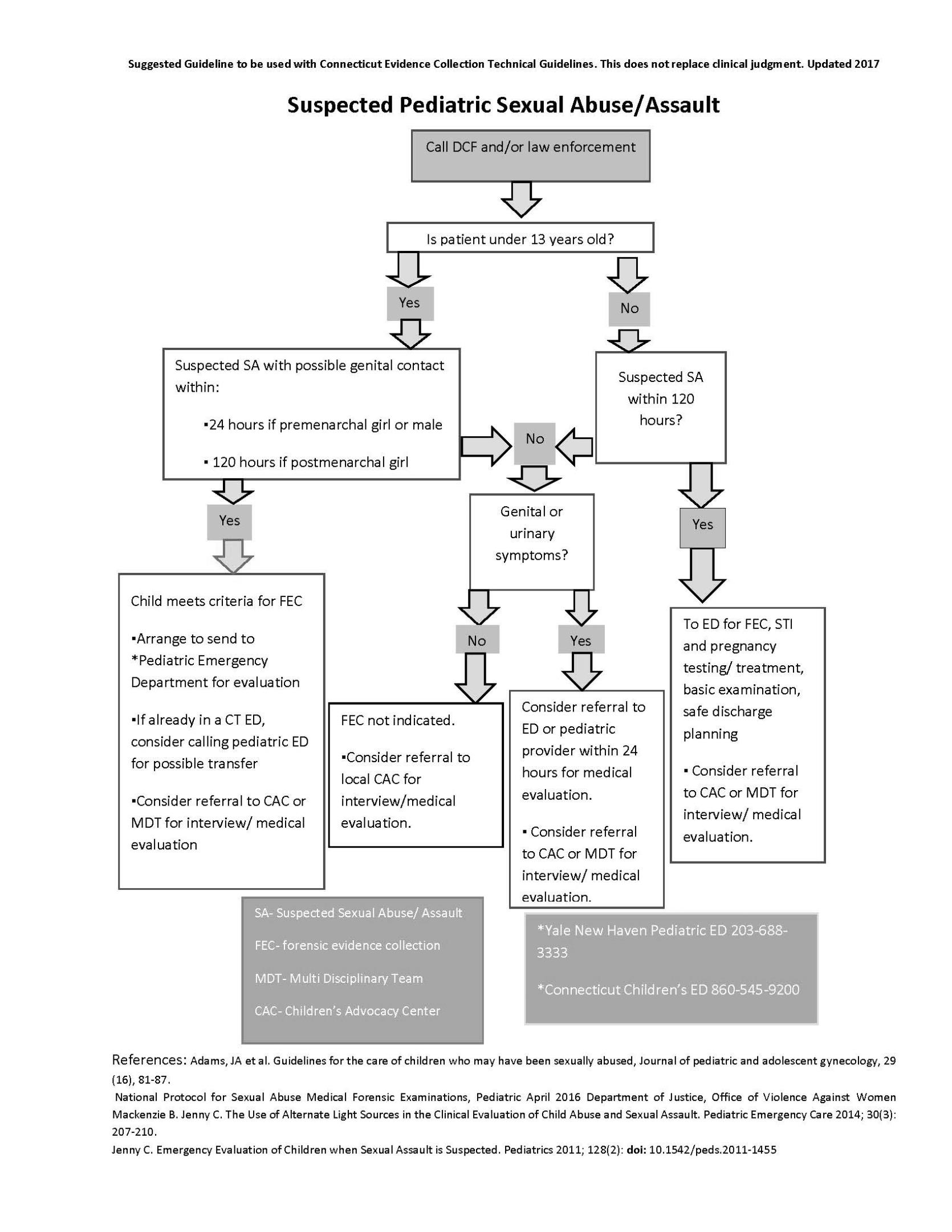
CT100B and CT400A Forms
CT100B:
-
Consent Form
-
Page 1: Medical Report and History
-
Page 1A: Medical Report and History (continued)
-
Page 1B: Medical Report and History (continued)
-
Page 2: Medical Report and History (final)
-
Page 3: Physical Exam: Non-genital
-
Page 4: Physical Exam: Non-genital (continued)
-
Page 5: Physical Exam: Genital
-
Page 6: Signature Page
-
Page 7: Checklist
-
Page 8: Discharge Instructions
CT400A:
-
Consent Form
-
Documentation
CT100B:
Consent Form: Authorization and Release of Payment
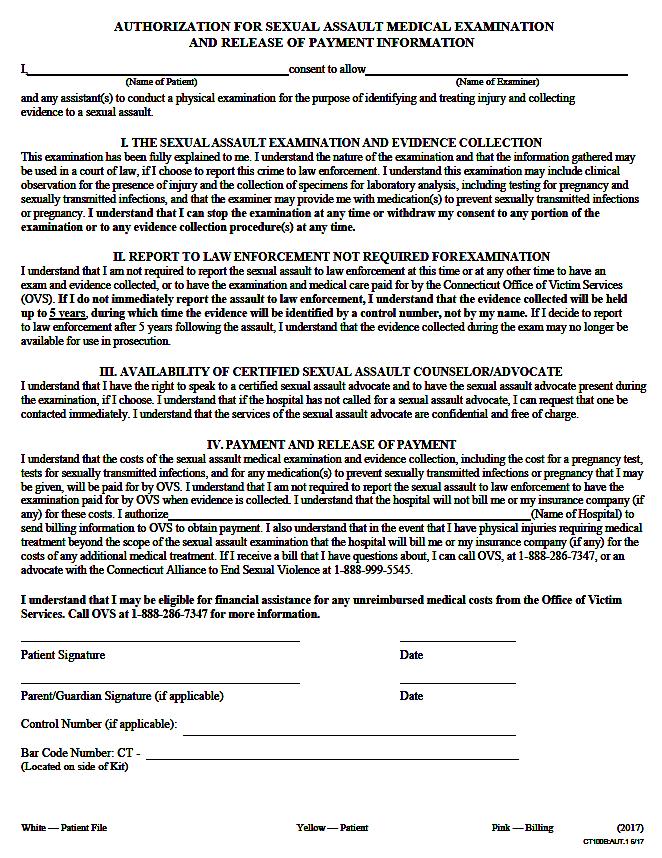 Page 1: Medical Report and History
Page 1: Medical Report and History
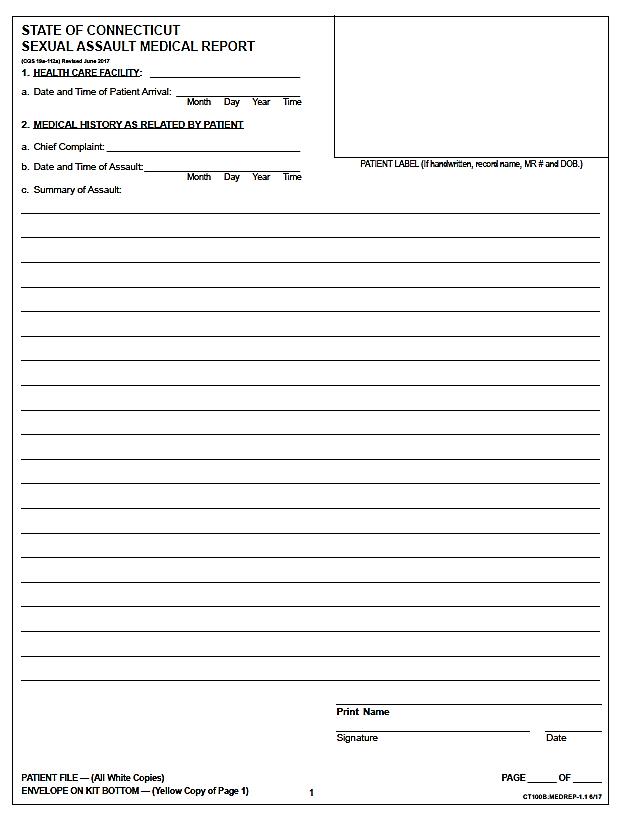
Page 1A: Medical Report and History (continued)
Page 1B: Medical Report and History (continued)
Page 2: Medical Report and History (final)
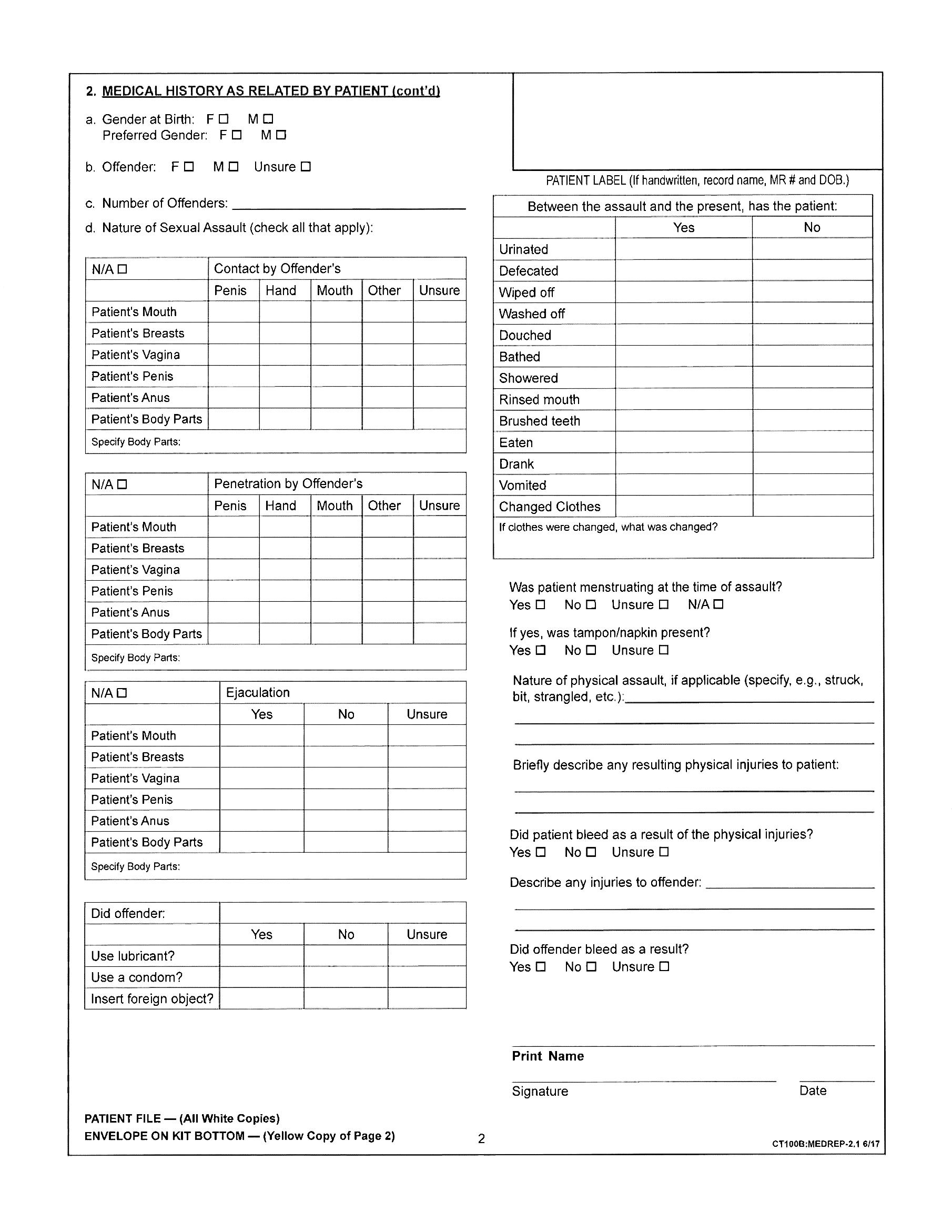
Page 3: Physical Exam: Non – genital
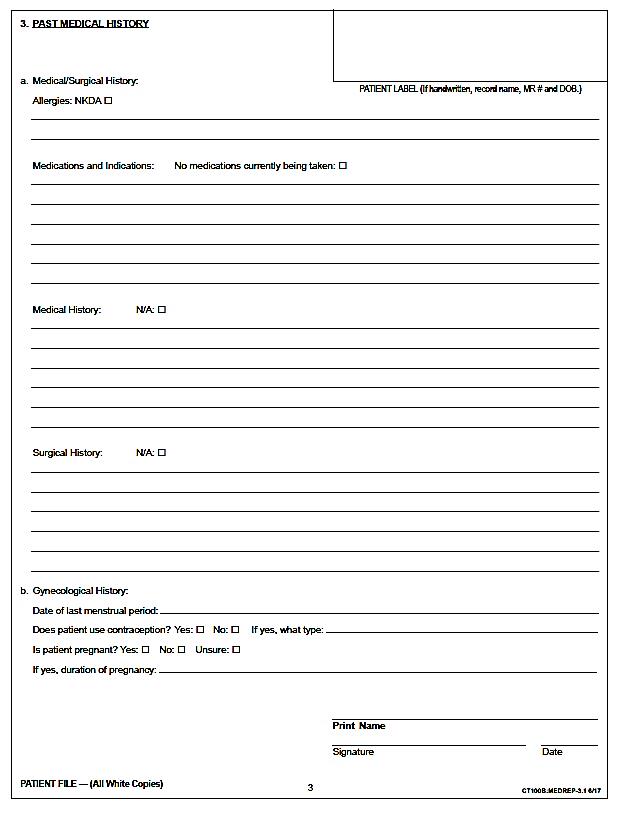
Page 4: Physical Exam: Non – genital (continued)
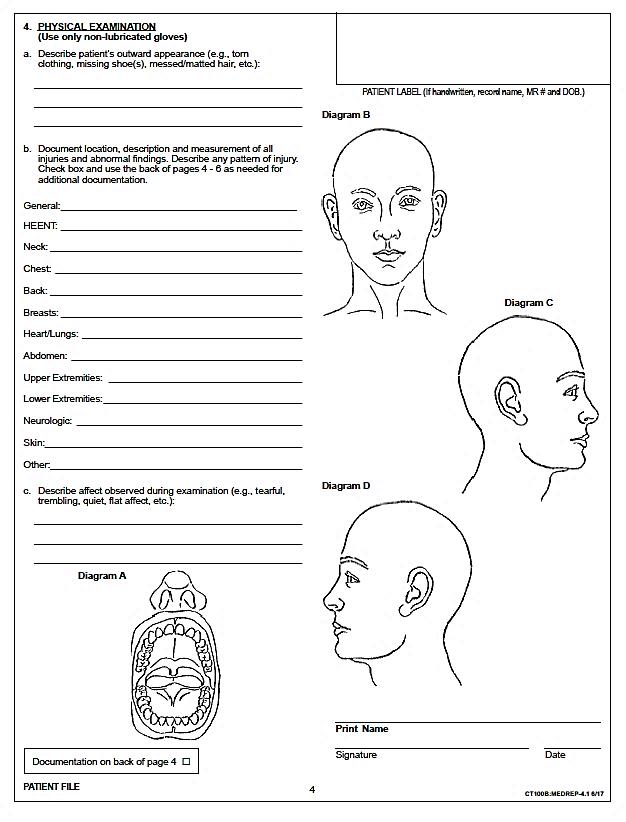
Page 5: Physical Exam: Genital
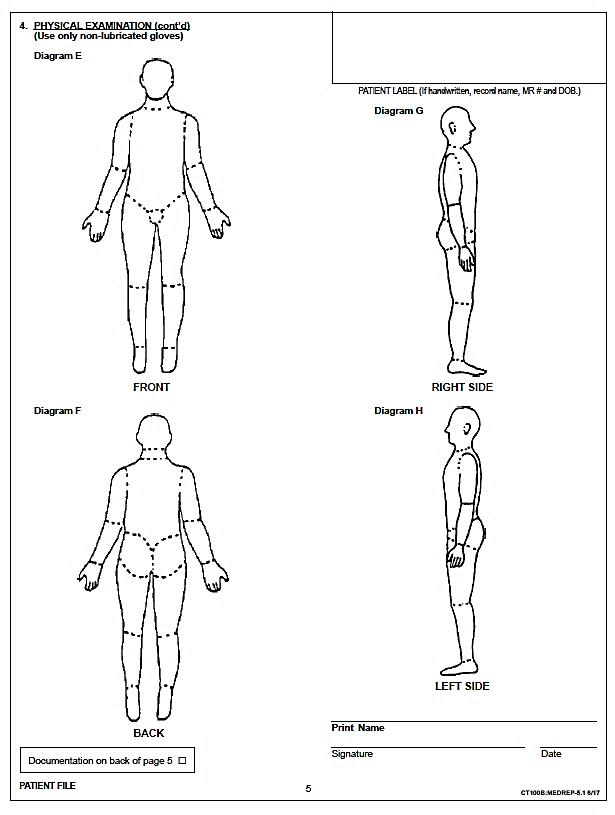
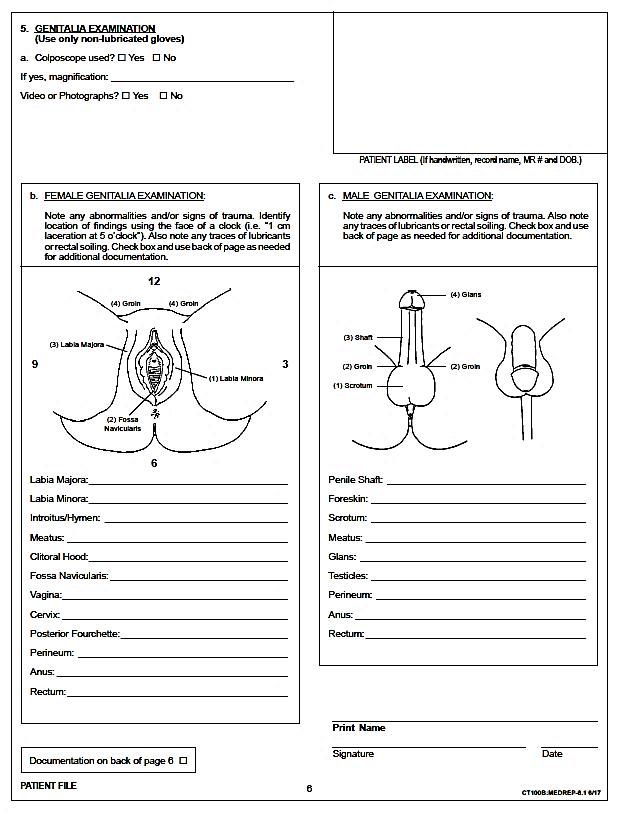
Page 6: Signature Page
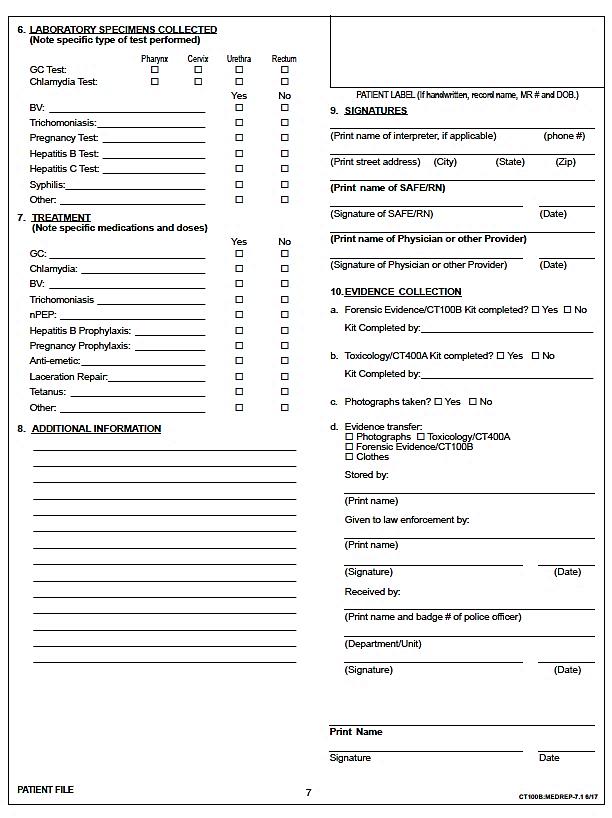
Page 7: Checklist
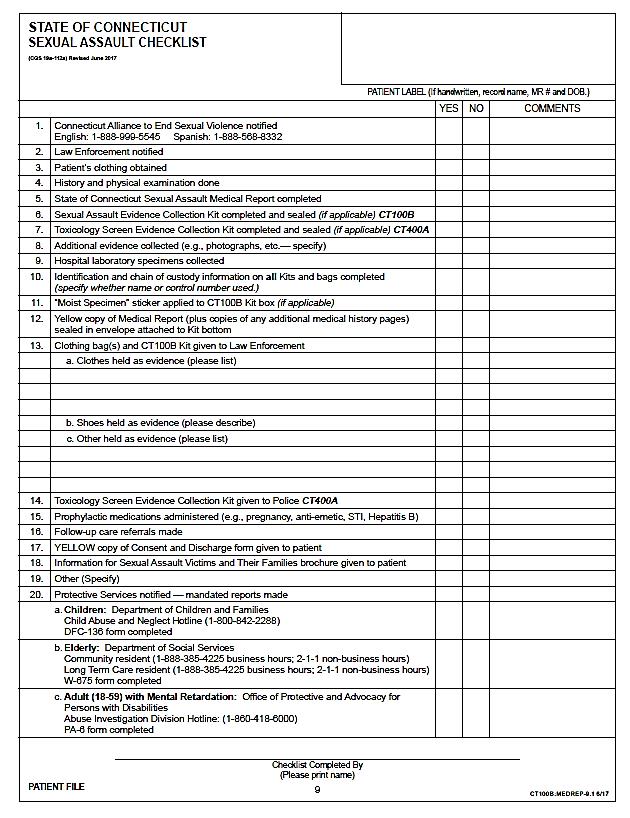
Page 8: Discharge Instructions
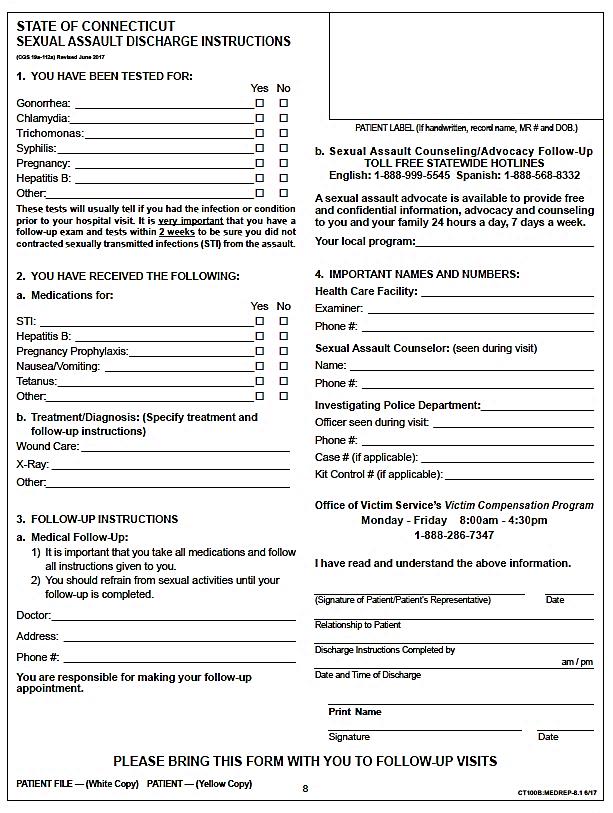
CT400A:
Consent Form
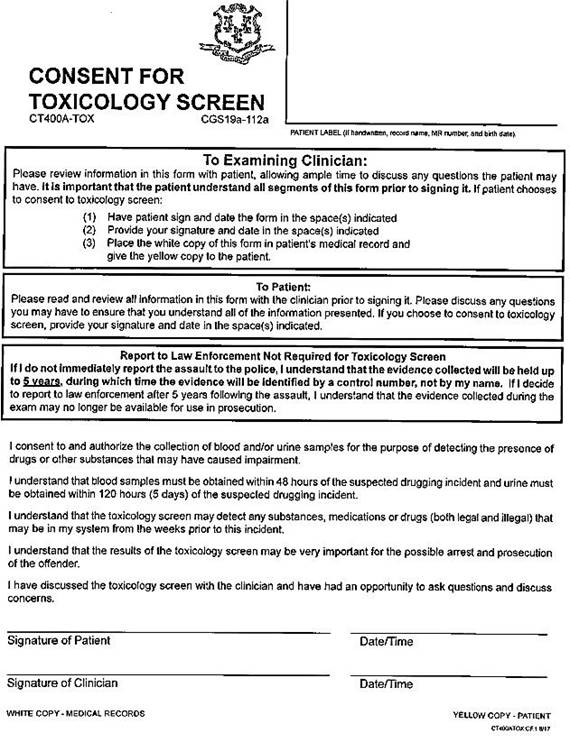
Documentation
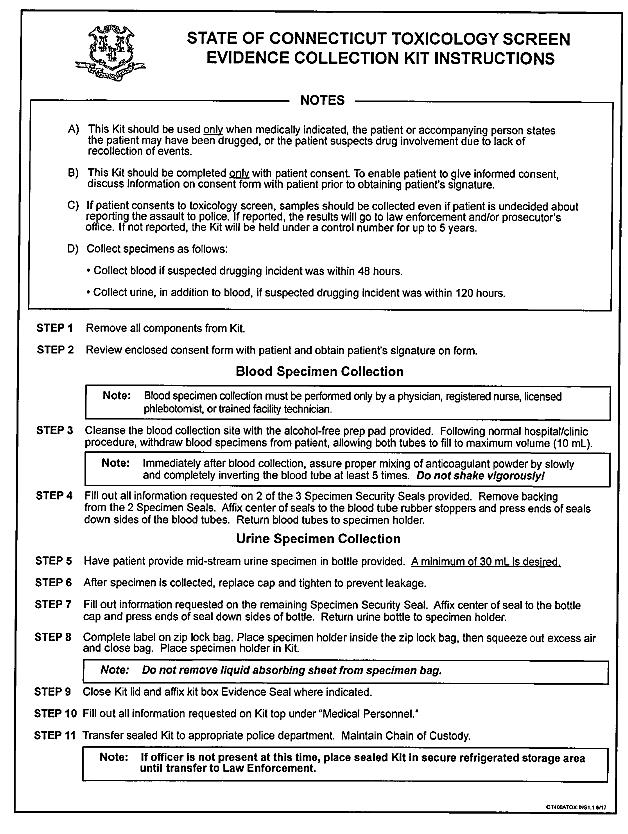
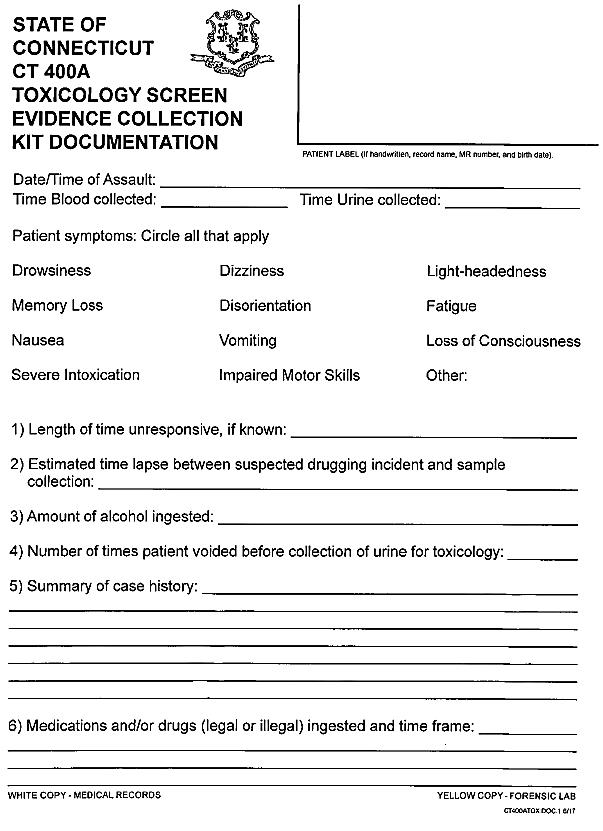
Appendix D
Strangulation Assessment
Recommendations for the Medical/Radiographic Evaluation of Acute Adult, Non-Fatal Strangulation
The Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations gratefully acknowledges Alliance for HOPE International, Bill Smock, MD, and Sally Sturgeon, DNP, SANE-A, for allowing us to reproduce, in part or in whole, the RECOMMENDATIONS for the MEDICAL/RADIOGRAPHIC EVALUATION of ACUTE ADULT, NON-FATAL STRANGULATION. The documents were accessed through the online Resource Library hosted by the Training Institute on Strangulation Prevention.
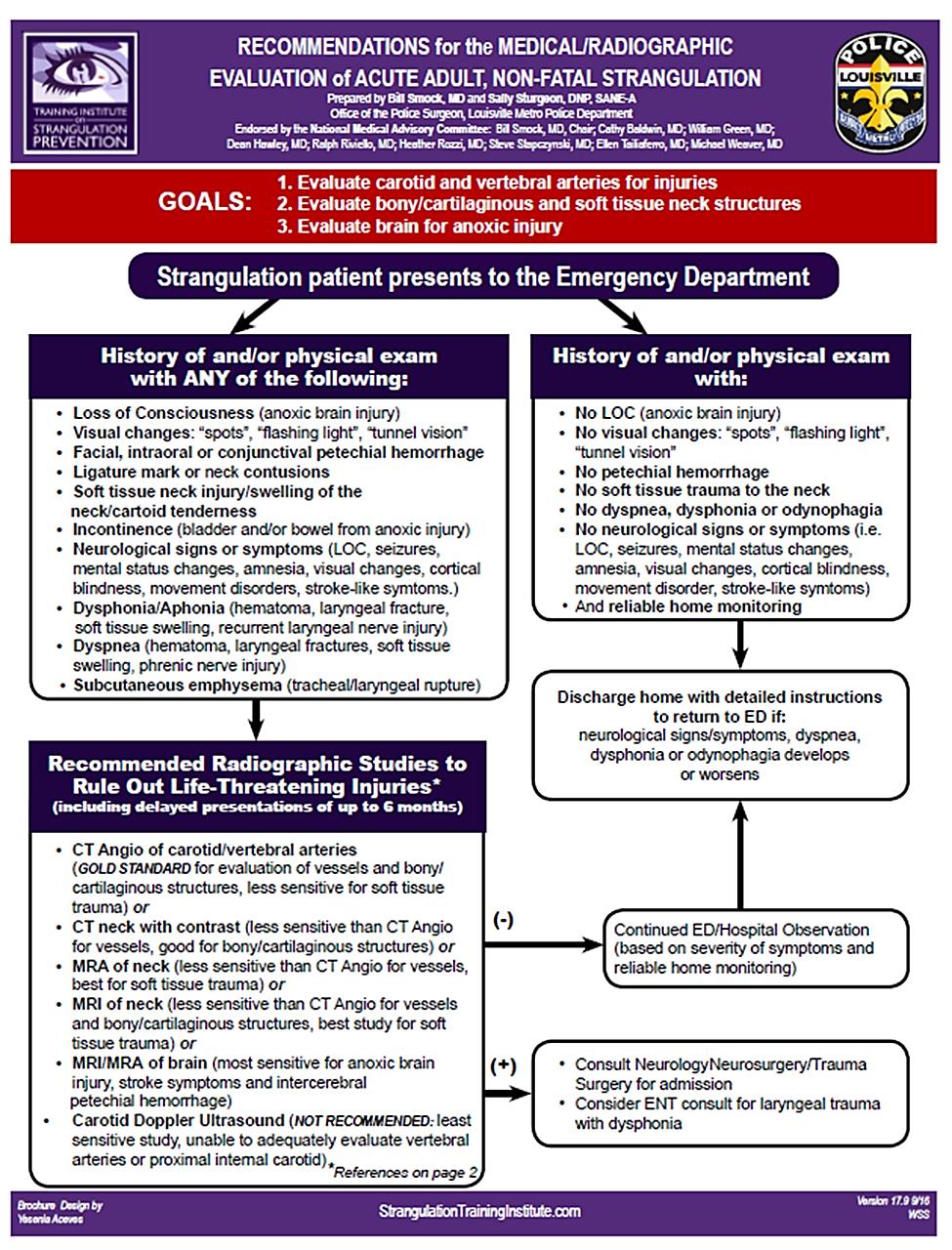
Appendix E
Mandatory Reporting Information and Forms
-
Abuse of Children – Reporting Information
-
DCF Form 136: Report for Suspected Child Abuse/Neglect
-
-
Abuse of Elderly (non-nursing home) – Reporting Information
-
Form W – 675: Report for Protective Services
-
-
Abuse of Elderly (nursing home) – Reporting Information
-
Form W – 410: Long-term Care Ombudsman Program
-
-
Abuse of Developmentally Disabled Adults – Reporting Information
-
Form PA- 6: Report of Suspected Abuse
-
Abuse of Children - Reporting Information
Child Abuse and Neglect Careline
505 Hudson Street
Hartford, CT 06106
Careline Phone Number for Oral Report: 1-800-842-2288
FAX: 860-560-7073
Abuse of Elderly (Non-Nursing Home) - Reporting Information
Protective Services for the Elderly
55 Farmington Avenue
Hartford, CT 06105-3730
In Connecticut: Phone for Oral Report (during business hours): 1-888-385-4225
In Connecticut: Phone for Oral Report (after business hours, on weekends and holidays): Infoline - 211
Out-of-State: Call Infoline at 1-800-203-1234
FAX: 860-424-5091
DSS Form W-675: Report for Protective Services
Abuse of Elderly (Nursing Home) - Reporting Information
Protective Services for the Elderly
55 Farmington Avenue
Hartford, CT 06105-3730
FAX: 860-424-5091
To: Mandatory Reporters for Residents of Nursing Homes Long Term Care Facilities
From: Dorian Long Program Administration Manager, Social Work Services
Date: September 24, 2015
Re: Review of Procedures and Mandated Reporting Form (W-410)
This memo is to update procedures and requirements regarding Connecticut General Statutes Sec.’s 17b-407 through 17b-408, which requires that suspected abuse, neglect, exploitation or abandonment of a resident in a long-term care facility be reported to the Commissioner of the Department of Social Services (effective 7/1/99).
The statute requires any mandatory reporter who has reasonable cause to suspect or believe that a long-term care resident has been abused, neglected, exploited or abandoned, report this information, or cause a report to be made, to the Social Work Division of the Department of Social Services within 72 hours of the incident. The following are definitions from the Connecticut State Statutes, Sec. 17b-450 that pertain to this reporting requirement:
Mandatory Reporters include “…Any physician or surgeon licensed under the provisions of chapter 370, any resident physician or intern in any hospital in this state, whether or not so licensed, and any registered nurse, licensed practical nurse, medical examiner, dentist, optometrist, chiropractor, podiatrist, social worker, clergyman, police officer, pharmacist, physical therapist, long-term care facility administrator, nurse’s aide or orderly in a long-term care facility, any person paid for caring for a patient in a long-term care facility, any staff person employed by a long-term care facility and any person who is a sexual assault counselor or a domestic violence counselor .”
Abuse “…includes, but is not limited to, the willful infliction of physical pain, injury or mental anguish, or the willful deprivation by a caregiver of services which are necessary to maintain physical or mental health.”
Neglect” refers to the failure or inability of an elderly person to provide for him or herself the services which are necessary to maintain physical and mental health or the failure to provide or arrange for provision of such necessary services by a caregiver.”
Exploitation “…refers to the act or process of taking advantage of an elderly person by another person or caregiver whether for monetary, personal, or other benefit, gain or profit.”
Abandonment “…refers to the desertion or willful forsaking of an elderly person by a caregiver or foregoing of duties or the withdrawal or neglect of duties and obligations owed an elderly person by a caregiver or other person.”
We receive numerous reports of resident-to-resident altercations. Incidents between residents need only be reported when the facility has made a determination that the resident who is the alleged “abuser” has the capability to take such action “intentionally, knowingly or recklessly” or, in the case of neglect, a person is acting with “criminal negligence,” as described in the CGS Penal Code Sec. 53a-3 Definitions:
A person acts “intentionally” with respect to a result or to conduct described by a statute defining an offense when his (her) conscious objective is to cause such result or to engage in such conduct.
A person acts “knowingly” with respect to conduct or to a circumstance described by a statute defining an offense when he (she) is aware that his conduct is of such nature or that such circumstance exists.
A person acts “recklessly” with respect to a result or to a circumstance described by a statute defining an offense when he (she) is aware of and consciously disregards a substantial and unjustifiable risk that such result will occur or that such circumstance exists. The risk must be of such nature and degree that disregarding it constitutes a gross deviation from the standard of conduct that a reasonable person would observe in the situation.
A person acts with “criminal negligence” with respect to or as a result of failing to perceive a substantial and unjustifiable risk that could occur. The risk must be of such nature and degree that the failure to perceive it constitutes a gross deviation from the standard of care that a reasonable person would observe in the situation.
Incidents meeting this legal standard, as a potential crime, must be reported to the police.
The determination of a resident’s capability to form intent should be made consistent with normal assessments of a resident’s condition and capabilities. Incidents among residents, which do not constitute abuse, should be addressed through facility assessment and care planning and incident reports to the State of Connecticut Department of Public Health as required by federal and state law.
As a reminder, the Office of the Long Term Care Ombudsman should continue to receive complaints directly from residents, family members or others acting on behalf of the resident. If a resident complains of “rough handling,” the facility is to ensure that resident is aware of the advocacy services provided by the Ombudsman. The facility should assist the resident in accessing the services of the Ombudsman.
Reports should be filed using the W-410 (Mandated Reporter Form) that is attached. This memo in no way impacts your reporting obligations to the Connecticut Department of Public Health.
If you have questions regarding the content of this memo, please call the Social Work Division at 1-888-385-4225. As a reminder, the fax number to send reports to is 860-424-5091. Telephone reports are not acceptable. Thank you.
Attachment
cc: Connecticut Department of Public Health
State LTC Ombudsman Form W-410
(Revised 5/06)
STATE OF CONNECTICUT
DEPARTMENT OF SOCIAL SERVICES
SOCIAL WORK DIVISION
55 Farmington Avenue
Hartford, CT 06105-3730
Phone: 1-888-385-4225
Fax: 860-424-5091
DSS Form W-410: Mandated Reporter Form for Long-Term Care Facilities

Abuse of Developmentally Disabled Adults - Reporting Information
Office of Protection and Advocacy for Persons with Disabilities
Abuse Investigation Unit
60B Weston Street
Hartford, CT 06120-1551
FAX: 860-297-4384
Form PA-6: Report of Suspected Abuse
Any physician or surgeon licensed under the provisions of chapter 370, any resident physician or intern in any hospital in this state, whether or not so licensed, any registered nurse, any person paid for caring for persons in any facility and any licensed practical nurse, medical examiner, dental hygienist, dentist, occupational therapist, optometrist, chiropractor, psychologist, podiatrist, social worker, school teacher, school principal, school guidance counselor, school paraprofessional, mental health professional, physician assistant, licensed or certified substance abuse counselor, licensed marital and family therapist, speech and language pathologist, clergyman, police officer, pharmacist, physical therapist, licensed professional counselor or sexual assault counselor or battered women's counselor, as defined in section 52-146k.
Do Those Mandated To Report Incur Liability?
No. Any person, institution or agency reporting in good faith is immune from any liability, civil or criminal.
Is There A Penalty For Not Reporting?
Yes. A person required to report who fails to do so shall be fined no more than $500.00.
What Is The Reporting Procedure?
1. An oral report must be made as soon as possible within seventy-two (72)hours to the Office of Protection and Advocacy, Abuse Investigation Division. In cases where the allegation results in death an oral report must be made within twenty-four (24) hours.
2. A written report must follow within five (5) additional calendar days of the oral report
3. All information as noted on the front of this form, if known by the reporter, must be reported.
What Must Be Reported?
1. Suspected or known abuse or neglect of adults with intellectual disability between the ages of 18 and 59 (in cases where the allegation results in death all persons over 18) inclusive, must be reported to the Office of Protection and Advocacy, Abuse Investigation Division. Abuse is defined as the willful infliction of physical pain or injury or the willful deprivation by a caretaker of services which are necessary to the person's health or safety. Neglect is defined as a situation where a person with intellectual disability is not able to provide for him/her the services which are necessary to maintain his/her physical and mental health or is not receiving such services from the caretaker.
2. If the person with intellectual disability is 17 years old or younger, a report must be made to the Department of Children and Families on a form supplied by them.
3. If the person with intellectual disability is not deceased and is 60 years old or older, a report must be made to the Department of Social Services, on a form supplied by them.
4. If the person with intellectual disability is between the ages of 18 and 59 inclusive, and lives in a nursing home, both the Office of Protection and Advocacy Abuse Investigation Division and The Department of Social Services Ombudsman Office must be contacted and two separate forms filed.
Do Private Citizens Have A Responsibility For Reporting?
A separate section of the law indicates that any person, in addition to those specifically mandated, having reasonable cause to believe that a person with intellectual disability is being or has been abused or neglected, may make written report to the Office of Protection and Advocacy.
What Is The Authority and Responsibility Of The Office of Protection and Advocacy?
1. The Office of Protection and Advocacy is responsible for the investigation of allegations of abuse of adults with intellectual disability between the ages of 18 and 59 inclusive (18 and over for allegations resulting in death.)
2. If it is determined that an adult with intellectual disability has been abused or neglected and/or is in need of protective services, the case shall be referred to the Department of Developmental Services for development and implementation of a plan of protective services. State or local police involvement will be requested if necessary.
3. If it is determined that a caretaker or other person has abused a person with intellectual disability such information shall be referred to the appropriate office of the State's Attorney, which shall conduct further investigation as may be deemed necessary and shall determine whether criminal proceedings should be initiated against such caretaker or other person in accordance with applicable state law.

Appendix F
The Connecticut Alliance to End Sexual Violence
-
Advocacy Services
-
Program Map
-
Program Contact Information
Advocacy – The Connecticut Alliance to End Sexual Violence
-
There are 9 sexual assault crisis programs in the state of CT. Each center provides the same core services:
-
24-hour toll free confidential hotline
-
Certified sexual assault victim advocates
-
Medical, police, and court accompaniment and advocacy
-
Support groups
-
Spanish-speaking & male advocates upon request
-
Information and referral
-
Community education
-
Short term supportive counseling
-
-
To contact the appropriate program please consult the program map and center information on the next two pages. To visit our website, go to: http://endsexualviolencect.org/
-
You can also call The Alliance’s hotline at 1-888-999-5545 from your hospital’s landline and you’ll be connected to your local center.
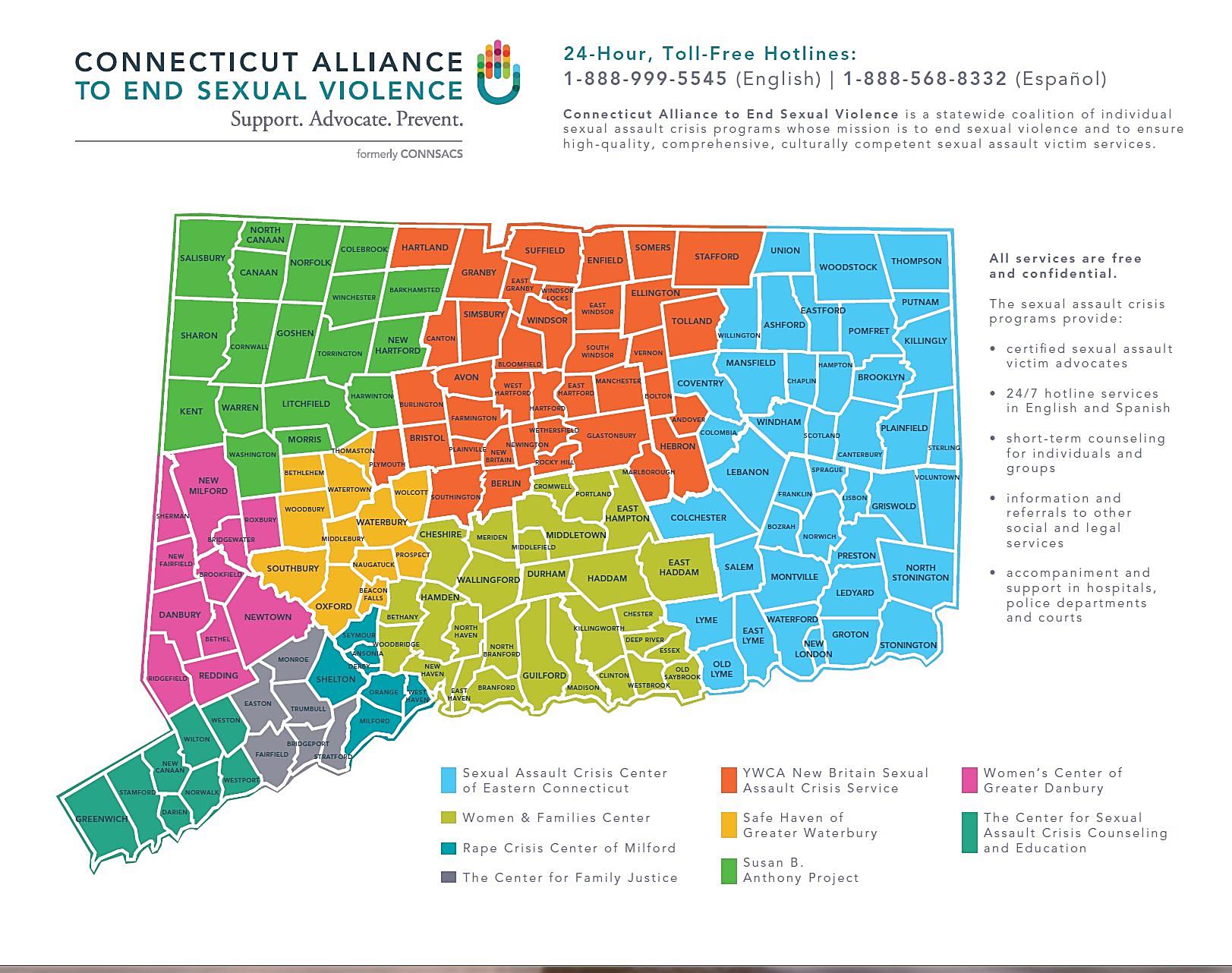

Appendix G
Intimate Partner Violence
-
Special Concerns Regarding Intimate Partner Sexual Violence
-
Intimate Partner Violence/Domestic Violence Victims
-
General Information and Initial Response
-
Counseling and Support
-
Program Map
Special Concerns Regarding Intimate Partner Sexual Violence (IPSV)
-
Intimate Partner Sexual Violence (IPSV) takes place within the context of domestic violence. An IPSV patient is or has been in a relationship in which sexual violence is part of a larger pattern of domination and control, with or without additional physical violence.[1]
-
Intimate Partner Violence (IPV) is a pattern of behaviors, not a single event or an isolated incident. Patient may have experienced sexual assault or other physical violence at the hands of their offender on previous occasions.
-
IPSV patients may be accompanied by their current or former partner or spouse. It is best to request the current or former partner or spouse to leave the room to conduct further assessment. Health care providers may cite hospital policy to allow further assessment to take place.
-
Patients who have been sexually assaulted by a current or former partner or spouse will likely not want the relationship to end, but for the violence to stop.
-
IPSV patients with children who are permitted no money or employment of their own may feel there is no escape.
-
Patients experiencing intimate partner sexual violence are socialized to see rape as involving non-consensual sex between two strangers. Patients may be reluctant to define a partner as a “rapist.”[2]
-
Sensitively asking questions specifically about IPSV is critical because the patient is unlikely to volunteer this information on their own.[3]
Intimate Partner Violence/Domestic Violence Victims
General Information
-
Intimate Partner Sexual Violence (IPSV) takes place within the context of domestic violence. An IPSV patient is or has been in a relationship with their offender and the sexual violence is part of a larger pattern of domination and control, with or without additional physical violence.[4]
-
IPSV patients include teens to elderly people (including same-sex partners) who are married, dating, or living together. Abuse by ex-spouses or former partners is also considered IPSV.
-
IPSV patients may have experienced multiple rapes. Although IPSV can be a one-time event, IPSV survivors suffer the highest frequency of multiple rapes.[5]
-
IPSV patient generally experience higher rates of severe injury.[6]
-
IPSV patients may experience deep shame of having continued the relationship, isolation, and ambivalence over their feelings for the offender, who may also be a partner, spouse, first love, or parent to her/his children.
Initial Response
-
IPSV patients generally are less likely to report sexual assaults or to seek medical care following a sexual assault due to societal views of what is or is not a sexual assault and the relationship between the patient and the offender.
-
Many IPSV patients will not consider what took place as, “rape.” A response should include open ended questions and be designed to facilitate disclosure using such words as sexual activity, intimate experience, and so forth.
-
IPSV patients may be more likely to have post-traumatic stress disorder symptoms, more pregnancies resulting from rape, and more sexually transmitted diseases.[7]
-
Victims of IPSV have higher levels of anal and oral rape—partner perpetrators commonly use these forms of assault to humiliate, punish and take “full” ownership of their partners.[8]
Counseling and Support
-
Call sexual assault crisis services as soon as possible and if possible alert them that the patient is experiencing IPSV to enhance the effectiveness of the counselor’s response.
-
The Alliance may be reached at 1-888-999-5545.
-
An IPSV patient may have profound shame regarding continuing the relationship after being sexually abused by a partner on multiple prior occasions.
Connecticut Coalition Against Domestic Violence (CCADV)
CCADV member organizations are Connecticut’s 18 domestic violence service organizations that provide critical support to victims of domestic violence. To contact a domestic violence advocate and for emergency shelter, counseling and other services, call the toll free domestic violence hotline at 888-774-2900 (English) or 844-831-9200 (Español). You may also call the direct hotline number of your local program, which is listed below. To visit our website, go to: http://www.ctcadv.org/
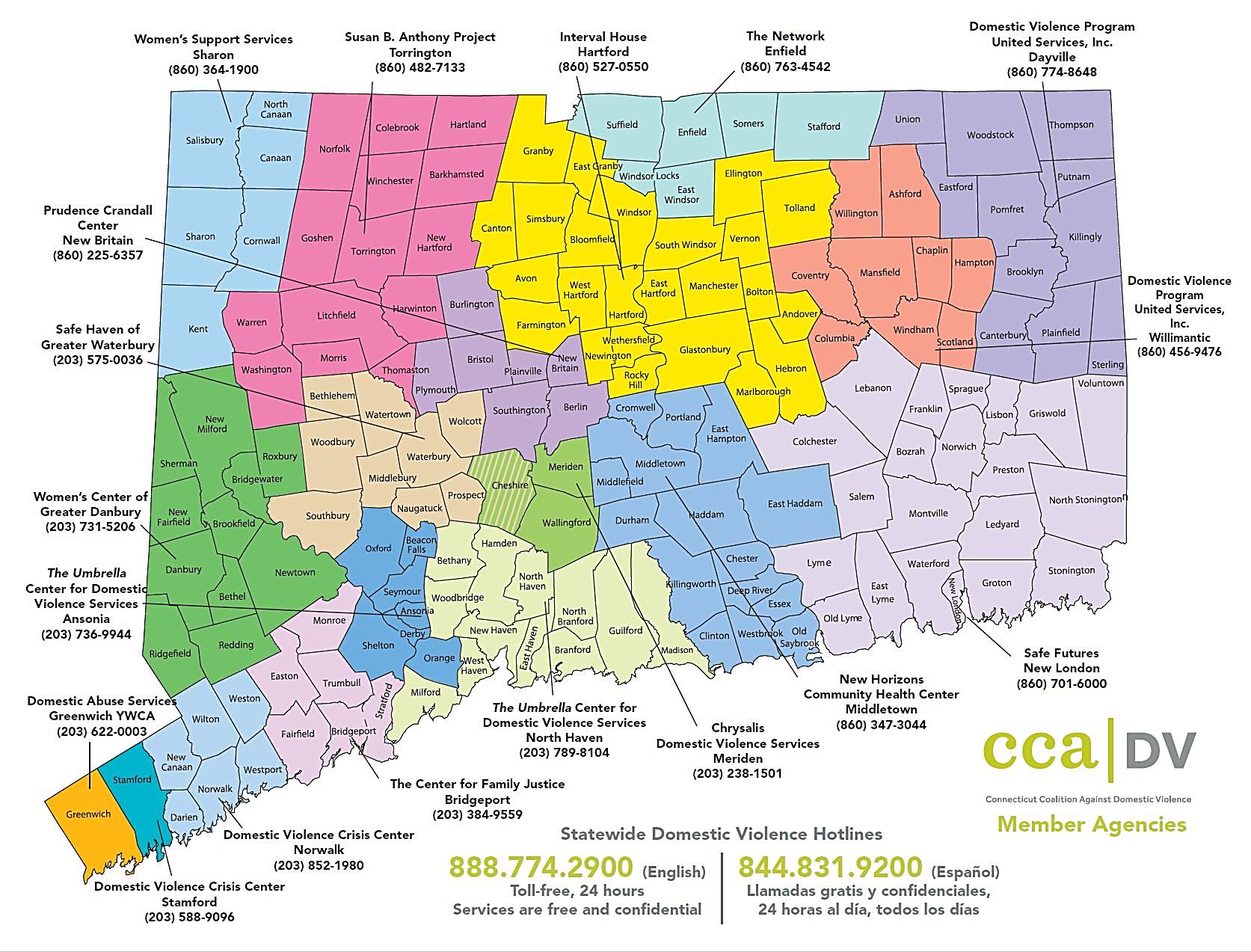
Appendix H
Office of Victim Services
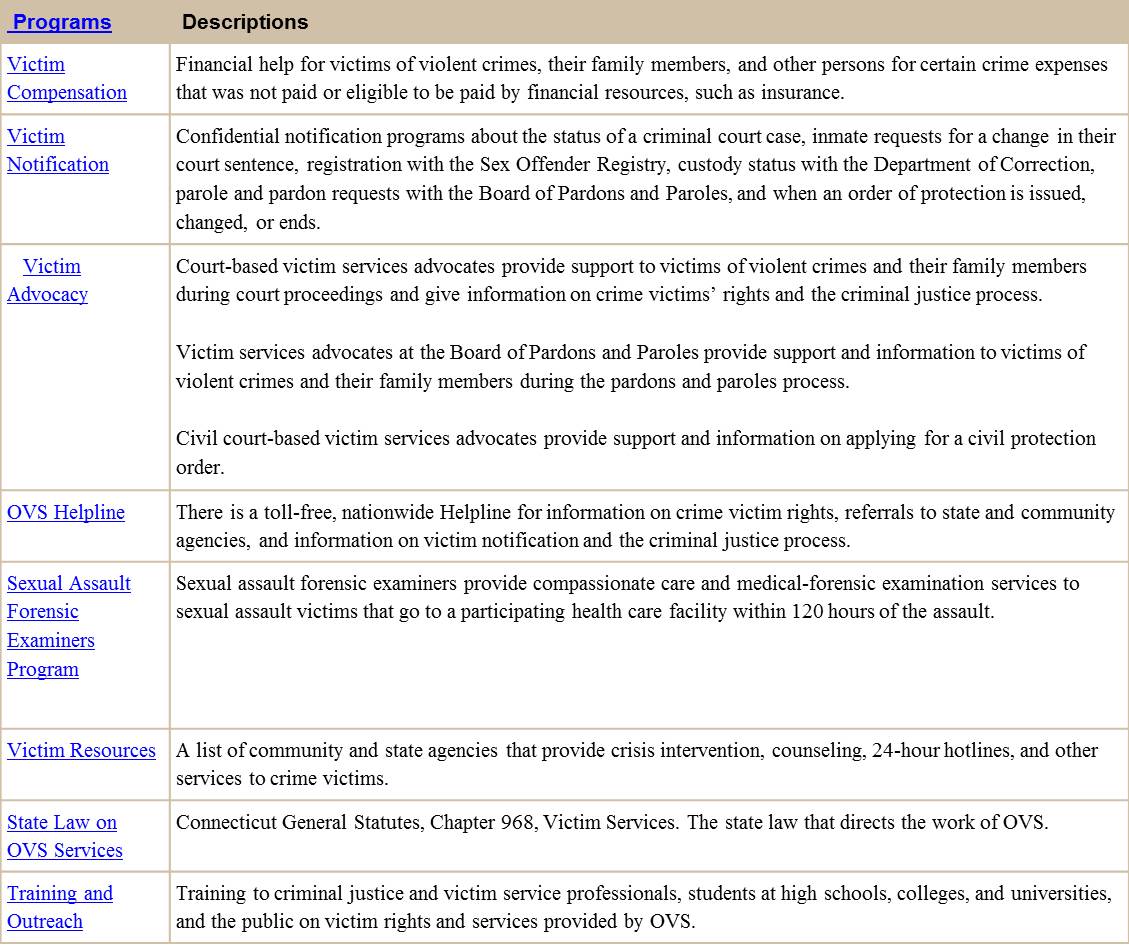
For more information about services and programs through the Office of Victim Services, go to: http://www.jud.ct.gov/crimevictim/
Appendix I
Billing
-
Forensic Kit Billing Information
-
Letter Bill Not Eligible for Reimbursement
-
UB for Billing
Appendix J
Compensation
![]()

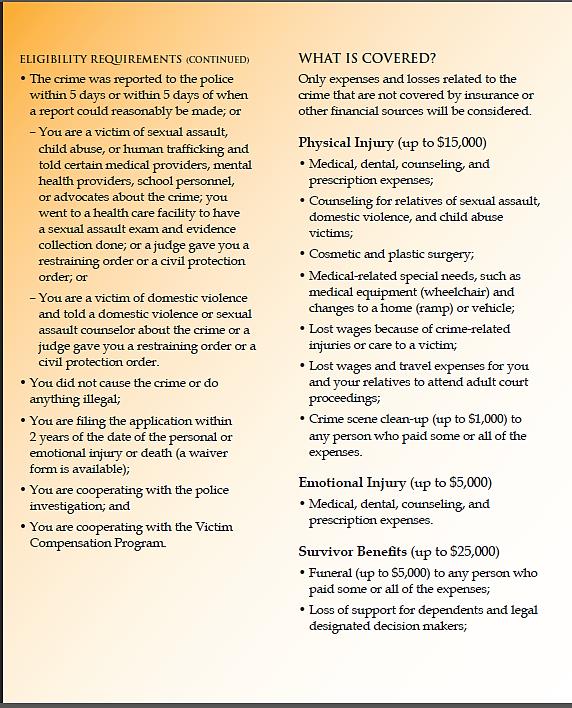
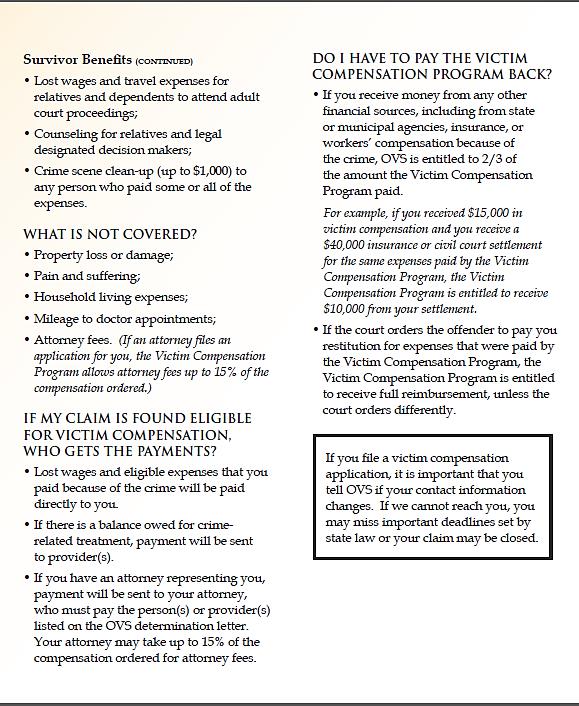
Appendix K
Connecticut General Statutes
-
Sec. 19a-112a. Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations. Protocol. Sexual assault evidence collection kit. Preservation of evidence. Costs. Training and sexual assault examiner programs
-
Sec. 19a-112e. Provision of emergency treatment to a victim of sexual assault. Standard of care
-
Sec. 19a-112g. Sexual assault forensic examiners. Responsibilities
-
Public Act 17-31. An Act Concerning Strengthening Laws Concerning Domestic Violence
Sec. 19a-112a. Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations. Protocol. Sexual assault evidence collection kit. Preservation of evidence. Costs. Training and sexual assault examiner programs.
(a) There is created a Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations composed of fourteen members as follows: The Chief State’s Attorney or a designee; the executive director of the Permanent Commission on the Status of Women or a designee; the Commissioner of Children and Families or a designee; one member from the Division of State Police and one member from the Division of Scientific Services appointed by the Commissioner of Emergency Services and Public Protection; one member from Connecticut Sexual Assault Crisis Services, Inc. appointed by its board of directors; one member from the Connecticut Hospital Association appointed by the president of the association; one emergency physician appointed by the president of the Connecticut College of Emergency Physicians; one obstetrician-gynecologist and one pediatrician appointed by the president of the Connecticut State Medical Society; one nurse appointed by the president of the Connecticut Nurses’ Association; one emergency nurse appointed by the president of the Emergency Nurses’ Association of Connecticut; one police chief appointed by the president of the Connecticut Police Chiefs Association; and one member of the Office of Victim Services within the Judicial Department. The Chief State’s Attorney or a designee shall be chairman of the commission. The commission shall be within the Division of Criminal Justice for administrative purposes only.
(b) (1) For the purposes of this section, “protocol” means the state of Connecticut Technical Guidelines for Health Care Response to Victims of Sexual Assault, including the Interim Sexual Assault Toxicology Screen Protocol, as revised from time to time and as incorporated in regulations adopted in accordance with subdivision (2) of this subsection, pertaining to the collection of evidence in any sexual assault investigation.
(2) The commission shall recommend the protocol to the Chief State’s Attorney for adoption as regulations in accordance with the provisions of chapter 54. Such protocol shall include nonoccupational post-exposure prophylaxis for human immunodeficiency virus (nPEP), as recommended by the National Centers for Disease Control. The commission shall annually review the protocol and may annually recommend changes to the protocol for adoption as regulations.
(c) The commission shall design a sexual assault evidence collection kit and may annually recommend changes in the kit to the Chief State’s Attorney. Each kit shall include instructions on the proper use of the kit, standardized reporting forms, standardized tests which shall be performed if the victim so consents and standardized receptacles for the collection and preservation of evidence. The commission shall provide the kits to all health care facilities in the state at which evidence collection examinations are performed at no cost to such health care facilities.
(d) Each health care facility in the state which provides for the collection of sexual assault evidence shall follow the protocol as described in subsection (b) of this section and, with the consent of the victim, shall collect sexual assault evidence. After the collection of any evidence, the health care facility shall contact a police department to receive the evidence. Not later than ten days after the collection of the evidence, the police department shall transfer the evidence in a manner that maintains the integrity of the evidence, to the Division of Scientific Services within the Department of Emergency Services and Public Protection or the Federal Bureau of Investigation laboratory. If the evidence is transferred to the division, the division shall analyze the evidence not later than sixty days after the collection of the evidence or, if the victim chose to remain anonymous and not report the sexual assault to the police department at the time of collection, shall hold the evidence for at least five years after the collection of the evidence. If a victim reports the sexual assault to the police department after the collection of the evidence, such police department shall notify the division that a report has been filed not later than five days after filing such report and the division shall analyze the evidence not later than sixty days after receiving such notification. The division shall hold any evidence received and analyzed pursuant to this subsection until the conclusion of any criminal proceedings. The failure of a police department to transfer the evidence not later than ten days after the collection of the evidence, or the division to analyze the evidence not later than sixty days after the collection of the evidence or after receiving a notification from a police department, shall not affect the admissibility of the evidence in any suit, action or proceeding if the evidence is otherwise admissible.
(e) (1) No costs incurred by a health care facility for the examination of a victim of sexual assault, when such examination is performed for the purpose of gathering evidence as prescribed in the protocol, including the costs of testing for pregnancy and sexually transmitted diseases and the costs of prophylactic treatment as provided in the protocol, and no costs incurred for a medical forensic assessment interview conducted by a health care facility or provider or by an examiner working in conjunction with a multidisciplinary team established pursuant to section 17a-106a or with a child advocacy center, shall be charged directly or indirectly to such victim. Any such costs shall be charged to the Forensic Sex Evidence Exams account in the Judicial Department.
(2) No costs incurred by a health care facility for any toxicology screening of a victim of sexual assault, when such screening is performed as prescribed in the protocol, shall be charged directly or indirectly to such victim. Any such costs shall be charged to the Division of Scientific Services within the Department of Emergency Services and Public Protection.
(f) The commission shall advise the Chief State’s Attorney on the establishment of a mandatory training program for health care facility staff regarding the implementation of the regulations, the use of the evidence collection kit and procedures for handling evidence.
(g) The commission shall advise the Chief State’s Attorney not later than July 1, 1997, on the development of a sexual assault examiner program and annually thereafter on the implementation and effectiveness of such program.
Sec. 19a-112e. Provision of emergency treatment to a victim of sexual assault. Standard of care.
(a) As used in this section:
(1) “Emergency contraception” means one or more prescription drugs used separately or in combination administered to or self-administered by a patient to prevent pregnancy, within a medically recommended amount of time after sexual intercourse and provided for that purpose, in accordance with professional standards of practice, and determined to be safe by the United States Food and Drug Administration.
(2) “Emergency treatment” means any medical examination or treatment provided in a licensed health care facility to a victim of sexual assault following an alleged sexual assault.
(3) “Medically and factually accurate and objective” means verified or supported by the weight of research conducted in compliance with accepted scientific methods and published in peer-reviewed journals, where applicable.
(4) “Victim of sexual assault” means any female person who alleges or is alleged to have suffered an injury as a result of a sexual offense.
(5) “Sexual offense” means a violation of subsection (a) of section 53a-70, section 53a-70a or 53a-70b, subsection (a) of section 53a-71, section 53a-72a or 53a-72b, subdivision (2) of subsection (a) of section 53a-86, subdivision (2) of subsection (a) of section 53a-87 or section 53a-90a, 53a-196a or 53a-196b.
(6) “Independent provider” means a physician licensed under chapter 370, a physician assistant licensed under chapter 370, an advanced practice registered nurse or registered nurse licensed under chapter 378, or a nurse-midwife licensed under chapter 377, all of whom are trained to conduct a forensic exam in accordance with the state of Connecticut Technical Guidelines for Health Care Response to Victims of Sexual Assault, published by the Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations pursuant to section 19a-112a.
(b) The standard of care for each licensed health care facility that provides emergency treatment to a victim of sexual assault shall include promptly:
(1) Providing each victim of sexual assault with medically and factually accurate and objective information relating to emergency contraception;
(2) Informing such victim of sexual assault of the availability of emergency contraception, its use and efficacy; and
(3) Providing emergency contraception to such victim of sexual assault at the facility upon the request of such victim, except that a licensed health care facility shall not be required to provide emergency contraception to a victim of sexual assault who has been determined to be pregnant through the administration of a pregnancy test approved by the United States Food and Drug Administration.
(c) In order to comply with the standard of care requirements prescribed in subsection (b) of this section, a licensed health care facility may contract with one or more independent providers to: (1) Ensure compliance at the facility with the standard of care requirements prescribed in said subsection (b), and (2) conduct at the facility a forensic exam of the sexual assault victim in accordance with the state of Connecticut Technical Guidelines for Health Care Response to Victims of Sexual Assault, published by the Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations pursuant to section 19a-112a.
(d) No licensed health care facility that provides emergency treatment to a victim of sexual assault shall determine such facility’s protocol for complying with the standard of care requirements prescribed in subsection (b) of this section on any basis other than a pregnancy test approved by the United States Food and Drug Administration.
Sec. 19a-112g. Sexual assault forensic examiners. Responsibilities.
(a) As used in this section, “sexual assault forensic examiner” means a registered nurse or advanced practice registered nurse licensed pursuant to chapter 378 or a physician licensed pursuant to chapter 370.
(b) A sexual assault forensic examiner may provide immediate care and treatment to a victim of sexual assault who is a patient in an acute care hospital and may collect evidence pertaining to the investigation of any sexual assault in accordance with the State of Connecticut Technical Guidelines for Health Care Response to Victims of Sexual Assault, published by the Commission on the Standardization of the Collection of Evidence in Sexual Assault Investigations pursuant to section 19a-112a. Services provided by a sexual assault forensic examiner shall be: (1) In accordance with the hospital’s policies and accreditation standards; and (2) pursuant to a written agreement entered into by the hospital, the Department of Public Health and the Office of Victim Services concerning the hospital’s participation in the sexual assault forensic examiners program. Nothing in this section shall be construed as altering the scope of the practice of nursing as set forth in section 20-87a.
Public Act 17-31. An Act Concerning Strengthening Laws Concerning Domestic Violence
Be it enacted by the Senate and House of Representatives in General Assembly
Sec. 3. Section 53a-64aa of the general statutes is repealed and the following is substituted in lieu thereof (Effective October 1, 2017):
(a) A person is guilty of strangulation or suffocation in the first degree when such person commits strangulation or suffocation in the second degree as provided in section 53a-64bb, as amended by this act, and (1) in the commission of such offense, such person (A) uses or attempts to use a dangerous instrument, or (B) causes serious physical injury to such other person, or (2) such person has previously been convicted of a violation of this section or section 53a-64bb, as amended by this act.
(b) No person shall be found guilty of strangulation or suffocation in the first degree and unlawful restraint or assault upon the same incident, but such person may be charged and prosecuted for all three offenses upon the same information. For the purposes of this section, "unlawful restraint" means a violation of section 53a-95 or 53a-96, and "assault" means a violation of section 53a-59, 53a-59a, 53a-59b, 53a-59c, 53a-60, 53a-60a, 53a-60b, 53a-60c, 53a-61 or 53a-61a.
(c) Strangulation or suffocation in the first degree is a class C felony.
Sec. 4. Section 53a-64bb of the general statutes is repealed and the following is substituted in lieu thereof (Effective October 1, 2017):
(a) A person is guilty of strangulation or suffocation in the second degree when such person restrains another person by the neck or throat or obstructs such other person's nose or mouth with the intent to impede the ability of such other person to breathe or restrict blood circulation of such other person and such person impedes the ability of such other person to breathe or restricts blood circulation of such other person.
(b) No person shall be found guilty of strangulation or suffocation in the second degree and unlawful restraint or assault upon the same incident, but such person may be charged and prosecuted for all three offenses upon the same information. For the purposes of this section, "unlawful restraint" means a violation of section 53a-95 or 53a-96, and "assault" means a violation of section 53a-59, 53a-59a, 53a-59b, 53a-59c, 53a-60, 53a-60a, 53a-60b, 53a-60c, 53a-61 or 53a-61a.
(c) Strangulation or suffocation in the second degree is a class D felony.
Sec. 5. Section 53a-64cc of the general statutes is repealed and the following is substituted in lieu thereof (Effective October 1, 2017):
(a) A person is guilty of strangulation or suffocation in the third degree when such person recklessly restrains another person by the neck or throat or obstructs such other person's nose or mouth and impedes the ability of such other person to breathe or restricts blood circulation of such other person.
(b) No person shall be found guilty of strangulation or suffocation in the third degree and unlawful restraint or assault upon the same incident, but such person may be charged and prosecuted for all three offenses upon the same information. For the purposes of this section, "unlawful restraint" means a violation of section 53a-95 or 53a-96, and "assault" means a violation of section 53a-59, 53a-59a, 53a-59b, 53a-59c, 53a-60, 53a-60a, 53a-60b, 53a-60c, 53a-61 or 53a-61a.
(c) Strangulation or suffocation in the third degree is a class A misdemeanor.
[1] IPSV Support Group: A Guide to Psychoeducational Support Groups for Survivors of Intimate Partner Sexual Violence, Washington Coalition of Sexual Assault Programs.
[2] Connections: A Biannual Publication of Washington Coalition of Sexual Assault Programs, Summer 2008.
[3] Marital Rape: New Research and Directions, February 2006.
[4] Ibid, Footnote 1.
[5] Connections: A Biannual Publication of Washington Coalition of Sexual Assault Programs, Summer 2008.
[6] IPSV Support Group: A Guide to Psychoeducational Support Groups for Survivors of Intimate Partner Sexual Violence, Washington Coalition of Sexual Assault Programs.
[7] U.S. Department of Justice, Office of Justice Programs, National Institute of Justice, January 2007.
[8] Connections: A Biannual Publication of Washington Coalition of Sexual Assault Programs, Summer 2008.