Pg 2 November 2023
Connecticut Epidemiologist Newsletter • November 2023 • Volume 43, No 8
Not Just for Travelers: ETEC in Connecticut, 2019 — 2022
Background
Enterotoxigenic Escherichia coli (ETEC) causes a toxin-mediated gastrointestinal illness that is characterized by cholera-like watery diarrhea that usually resolves after 3-5 days but may last for several weeks. Complications are mainly from dehydration, which can be life-threatening. It is the most commonly diagnosed cause of diarrhea in US international travelers. Prior to the widespread availability of specific diagnostic tests, it was estimated that in the US there were approximately 40,000 infections annually with the majority related to international travel (1).
In the past 8 years, a culture-independent diagnostic test for ETEC toxins has become readily available to clinical laboratories as part of a multi-pathogen panel using PCR (FilmArray® gastrointestinal panel; BioFire® Diagnostics, Salt Lake City, UT). It has been adopted by some Connecticut (CT) laboratories for routine testing of patients with diarrheal illness. Other laboratories are not able to test for ETEC routinely. Recognizing the opportunity to conduct surveillance to describe the epidemiology of ETEC in CT, ETEC was made laboratory-reportable in 2019. The objective of this analysis is to describe the epidemiology of detected ETEC cases and to estimate the degree of under detection of ETEC among persons seeking clinical consultation for diarrhea given that a minority of clinical laboratories routinely perform testing that could detect ETEC in CT.
Epidemiologists from the CT Department of Public Health first contact the clinician of record, then the patient for each reported positive ETEC test. Data are collected on patient demographics, symptoms and international travel in the 7 days before the onset of illness using a standardized form. To determine potential under detection of cases, laboratories were classified as those routinely testing for ETEC or not based on an annual laboratory survey conducted by the Connecticut Emerging Infections Program. The average percentage of all statewide reported Salmonella, Campylobacter, and Shiga toxin-producing E. coli (STEC) infections, pathogens for which all CT-based clinical laboratories routinely test, diagnosed at labs testing for ETEC was determined and used to calculate estimates of ETEC under detection statewide. A total of 300 cases of ETEC were reported from 2019-2022 from the five (of 32) clinical laboratories that routinely performed the multiplex test that could detect ETEC. Of the approximately 90% of cases for whom clinical data were available, 96% reported diarrhea, 29% fever and 16% bloody diarrhea; 26% were hospitalized and none died.
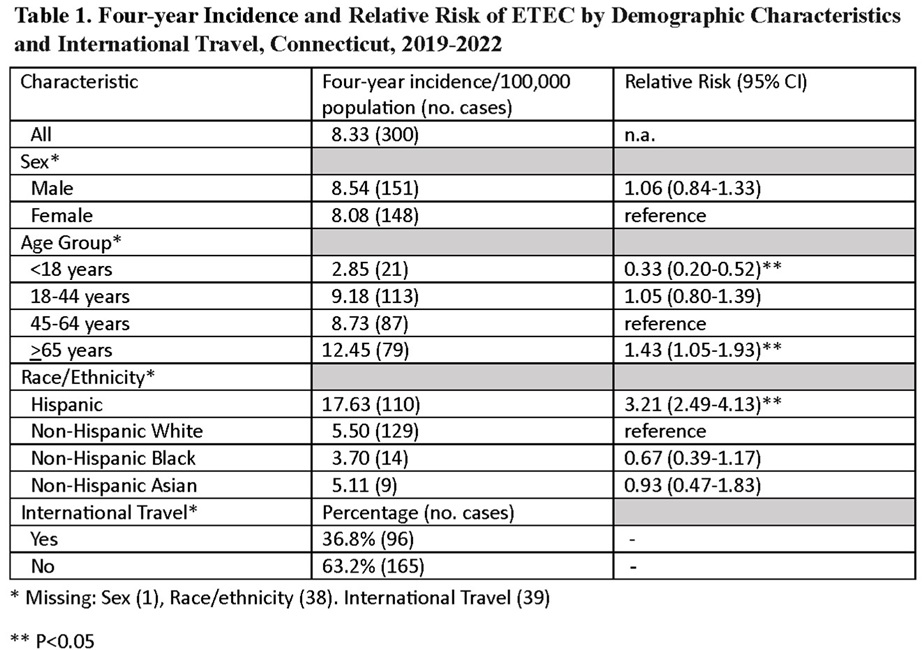
Overall four-year incidence was 8.33 per 100,000 population. Groups at highest risk were Hispanics (relative risk [RR] 3.21, 95% confidence interval [CI] 2.49-4.13 vs non-Hispanic White) and those >65 years old (RR 1.43, 95% CI 1.05-1.93 vs 45-64 years old). Children <18 years had the lowest relative risk (RR 0.33, 95%CI 0.20-0.52 compared to 45-64 year olds). Of the 261 cases with travel information, 36.8% had international travel in 7 days before symptom onset and 63.2% did not (Table 1). International travel destinations were mostly (69%) to Mexico, the Dominican Republic or Central and South American countries.
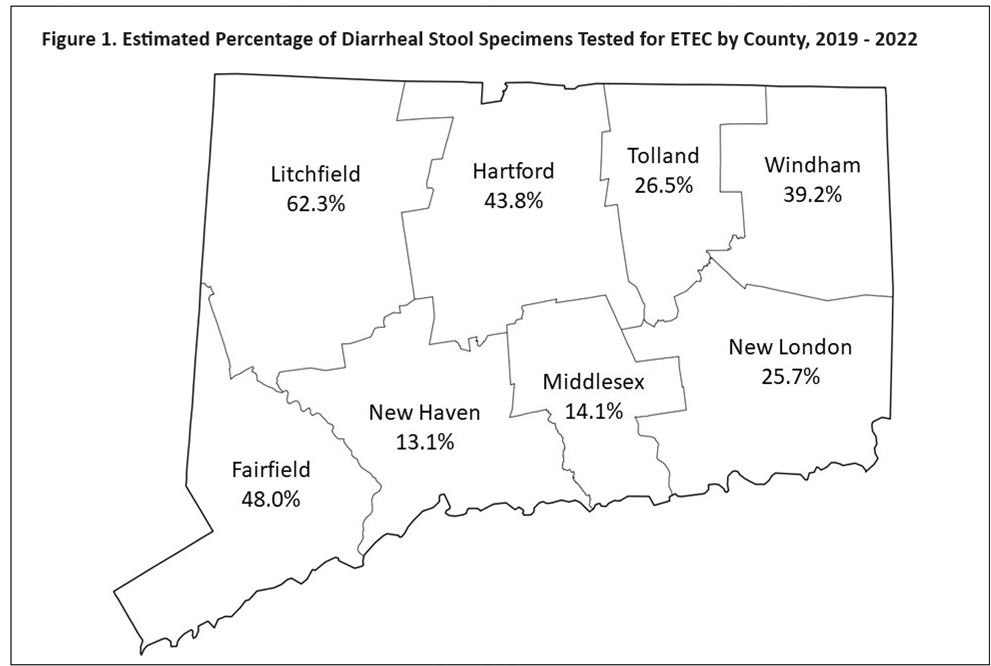
The proportions of Salmonella, Campylobacter, and STEC infections diagnosed at laboratories with ETEC testing capacity averaged 35.1% statewide. There were marked differences in this proportion by county, with the highest proportions in Litchfield 62.3%) and Fairfield (48.0%) and the lowest in New Haven (13.3%) and Middlesex (14.1%) counties (Figure 1).
When the estimate that only 35.1% of diarrheal cases seeking medical attention got tested for ETEC is applied to the 300 cases identified, it is possible that there could have been 855 cases identified statewide had all clinical laboratories been routinely testing diarrheal specimens for it. Of these, 530 (63.2% x 855) would be estimated to be domestically acquired.
Discussion
Recently in CT, domestically-acquired ETEC infection has consistently been more common than travel-associated. A study in Minnesota covering 2016-17 had a similar finding, in which 57% of cases had no international travel; Hispanics and adults were also at highest risk (2).
Although ETEC is well recognized as a cause of traveler’s diarrhea, the burden of domestically-acquired cases appears to be underappreciated. The Centers for Disease Control and Prevention ETEC webpage (3) does not mention its possible importance in the US, despite periodic domestically-acquired outbreaks such as the one described in this CT Epidemiologist issue. In CT, with routine testing, domestically acquired ETEC, estimated to be 530 cases, would be more common than STEC (459 cases from 2019-2022) as a cause of diarrhea needing medical attention.
While ETEC is currently under detected throughout Connecticut, testing for it is disproportionately lacking in laboratories serving residents of New Haven and Middlesex Counties. In these counties, the importance of locally-acquired ETEC is more likely to be unknown, other diagnoses requiring different treatment unnecessarily entertained and outbreaks missed.
Based on these findings, ETEC infection should continue to be under public health surveillance in CT. Efforts should be made to increase testing by both clinical laboratories and healthcare providers. Future goals of surveillance would include identification of exposure factors, including why ETEC is more common among Hispanics and less common among children.
ETEC infection occurs when a person eats food, or drinks water or ice contaminated with ETEC bacteria. Human or animal wastes (e.g., feces) are the ultimate source of ETEC contamination (3). Outbreaks in the US have often been attributed to vehicles such as salads, sometimes contaminated by an ill food handler (4). Until more is known about transmission patterns in the US, prevention should include washing all food and vegetables to be consumed raw and exclusion of food preparers with acute gastrointestinal illness, both inside and outside the home, until they are asymptomatic.
Reported by
N Bramlitt, MPH, J Hadler, MD, L Niccolai, PhD, Connecticut Emerging Infections Program, Yale School of Public Health
Acknowledgements
Connecticut FoodNet and FoodCore staff, especially Megan Fitzsimmons for analytic help.
References
1. Scallan E et al. Foodborne illness acquired in the United States-major pathogens. Emerg Infect Dis. 2011; 17: 7–15.
2. Buuck S, Smith K, et al. Epidemiology of enterotoxigenic Escherichia coli infection in Minnesota, 2016–2017. Epidemiology and Infection. 2020; 148, e206, 1–7. https://doi.org/10.1017/3.CDC (2014, December 1). Enterotoxigenic E. coli (ETEC). Retrieved from https://www.cdc.gov/ecoli/etec.html.
4. Devasia RA, Jones TF, et al. Endemically acquired foodborne outbreak of enterotoxin-producing Escherichia coli serotype O169:H41. Am J Med. 2006; 119(2):168.e7-10. doi: 10.1016/j.amjmed.2005.07.063. PMID: 16443428.
This page last updated 12/05/2023.