Pg1 July 2023
Connecticut Epidemiologist Newsletter • July 2023 • Volume 43, No 5Potential Impact of Higher Valency Conjugate Vaccines on Invasive Pneumococcal Disease in Connecticut
Invasive pneumococcal disease (IPD) is a leading cause of pneumonia, sepsis, and meningitis in children and adults (1). In 2019, there were an estimated 30,300 cases and 3,250 deaths caused by IPD in the United States. Subsequently, in 2020, during the first year of the COVID-19 pandemic, national case (17,680) and death (2,580) estimates decreased by 42% and 21% respectively due to pandemic associated non-pharmaceutical interventions (2,3).
People at high risk for IPD include children <5 and adults ≥65 years of age. In 2000, the Advisory Committee on Immunization Practices (ACIP) recommended the use of a 7-valent pneumococcal conjugate vaccine (PCV7) for infants and young children. In 2010, a 13-valent vaccine (PCV13) replaced PCV7 in the pediatric vaccine schedule. Routine pediatric use of these vaccines directly reduced the IPD burden in children. It also reduced disease in adults ≥65 years of age indirectly by enhancing community-level immunity (1). In 2022, a new 15-valent vaccine (PCV15) was added to the pediatric schedule as an alternative to PCV13. Subsequently, in June 2023, ACIP endorsed the use of either PCV15 or a newly licensed 20-valent vaccine (PCV20) for routine vaccination of children aged 2–23 months.
Routine use of PCV13 in series with the 23-valent pneumococcal polysaccharide vaccine (PPSV23) was recommended for adults ≥65 years of age starting in 2014. In 2019, the ACIP downgraded their guidance concerning PCV13 and recommended shared clinical decision-making rather than routine use in this age group (4). This was in part due to a lack of evidence that the use of PCV13 in adults ≥65 years of age further reduced disease beyond that due to community-level immunity caused by routine pediatric use. Subsequently, in October 2021, ACIP recommended routine use of either PCV20 alone or PCV15 in series with PPSV23 for all adults ≥65 years of age.
The Connecticut Department of Public Health (DPH) identifies IPD cases (people with Streptococcus pneumoniae isolated from a normally sterile site) through statewide active surveillance as part of the Active Bacterial Core Surveillance project. IPD is reportable to DPH by both physicians and laboratories. Isolates are routinely sent to CDC for serotyping. This article describes annual IPD incidence (per 100,000) in high-risk age groups from 2014–2021 by type including PCV15/nonPCV13 (22F and 33F) and PCV20/nonPCV15 (8, 10A, 11A, 12F, 15B, and 15C due to cross-reactivity) serotypes. The percent of IPD cases caused by PCV15/nonPCV13 and PCV20/nonPCV15 was calculated as an indicator of the potential for reduction in IPD incidence through the use of higher valency vaccines.
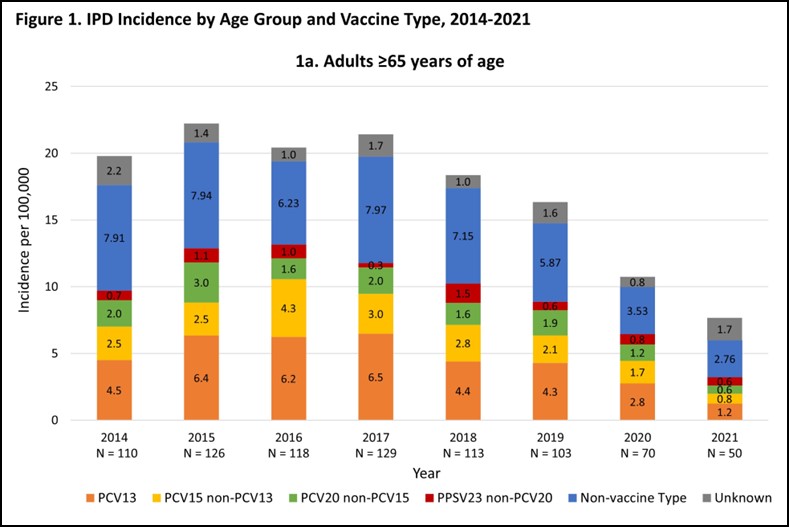
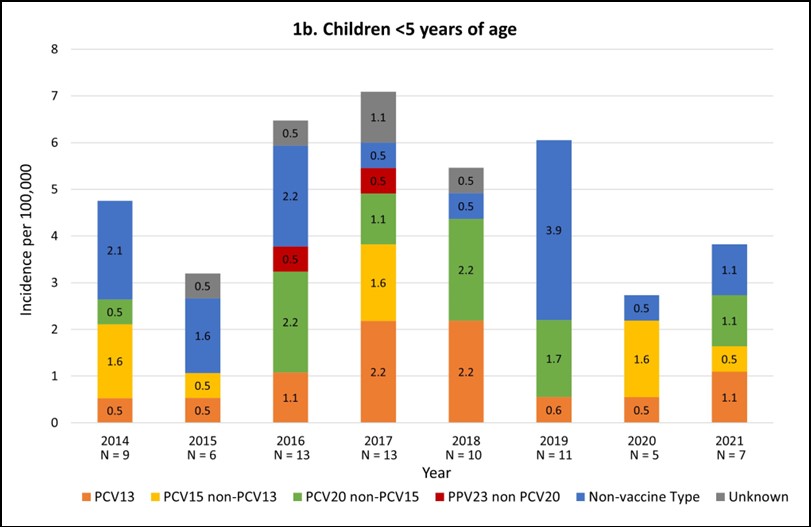
During 2014–2021, 1762 IPD cases were identified of which 819 (46%) were adults aged ≥65 years and 74 (4%) were children aged <5 years. Isolates were available for serotyping for 751 (92%) of adults and for 69 (93%) of children. Among adults aged ≥65 years, IPD incidence ranged from 16.3 to 22.2 per 100,000 during 2014–2019 (average annual incidence 19.6) and then decreased 52.8% through 2021 (16.3 in 2019 to 7.7 in 2021). Incidence of PCV20/non PCV15 disease in these adults averaged 2.0 per 100,000 during 2014–2019 (range 1.6 to 3.0) followed by a 68.4% decrease (1.9 in 2019 to 0.6 in 2021). Incidence of PCV15/nonPCV13 disease averaged 2.9 per 100,000 during 2014–2019 (range 2.1 to 4.3) followed by a 61.9% decrease (2.1 in 2019 to 0.8 in 2021). Among children aged <5 years, overall incidence ranged from 3.2 to 7.1 per 100,000 between 2014–2019 (average annual incidence 5.6) but then decreased 55.7% in 2020 (6.1 in 2019 to 2.7 in 2020). PCV15/nonPCV13 and PCV20/nonPCV15 incidence in children had no clear trend between 2014–2021 with average annual incidence of 0.6 and 0.9 per 100,000, respectively. [Figure 1a-b]
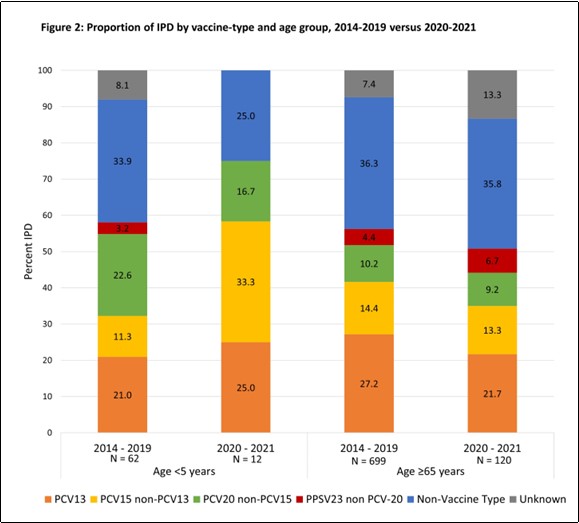
During 2020–2021, the proportion of adults aged ≥65 years with PCV15/nonPCV13 and PCV20/nonPCV15 type disease were 13.3% and 9.2% respectively with similar proportions seen during the 2014–2019 pre-pandemic period. Among children aged <5 years, the proportions of PCV15/nonPCV13 and PCV20/nonPCV15 type disease in 2020–2021 were 33.3% and 16.7% respectively. Although the proportion of PCV20/nonPCV15 type disease in children in 2020–2021 was similar to that in the pre-pandemic period, the proportion of PCV15/nonPCV13 type disease was 195% higher (33.3% in 2020–2021 versus 11.3% in 2014–2019). [Figure 2]
Discussion
In Connecticut, IPD rates decreased in both children and adults at the onset of the COVID-19 pandemic in 2020, and, as of 2021, have not returned to pre-pandemic levels. This pattern is consistent with that seen in other states and has been attributed to COVID-19 related non-pharmaceutical interventions (3). Assuming vaccine efficacy and uptake is high, the replacement of PCV13 with PCV15 or PCV20 in the pediatric vaccination schedule, as well as routine older adult vaccination with PCV15 or PCV20, has the potential to further reduce IPD burden in 2022 and beyond. Although the proportion of IPD due to PCV15 and PCV20 types remained stable among adults during 2014–2021, an increase in the proportion of PCV15/nonPCV13 type IPD was seen in children during the pandemic. If this pattern continues, the potential beneficial impact of the higher valency vaccines in this age group could be increased. However, low case counts among children in 2020–2021 (n=12) make interpretation of this finding limited.
The 2021 National Immunization Survey found that 92.8% of children in Connecticut received four PCV doses by 24 months as recommended by ACIP [5]. Continued high vaccination coverage among Connecticut children using the new higher valency vaccines is essential to further decrease pediatric IPD. Among Connecticut adults ≥65 years, 72.9% are estimated to have had a pneumococcal vaccine according to the 2021 Behavioral Risk Factor Surveillance System (6). However, this survey did not distinguish between receipt of PCV13 or PPSV23. In July 2022, all doses of vaccine administered to people of any age in Connecticut became reportable via CT Wiz, which is the immunization information system in Connecticut. This should make it possible to monitor the uptake of higher valency PCVs in adults aged ≥65 years.
Our analyses did not consider the vaccination status of individual case patients. Some may not have received the recommended vaccine(s) for their age group prior to IPD illness onset. Further analyses are needed to determine if vaccine failures have contributed to continued low levels of PCV13-type disease particularly among the pediatric age group.
Continued IPD surveillance is needed to monitor potential changes in disease burden that may emerge in PCV15, PCV20 and non-vaccine serotypes as the COVID-19 pandemic wanes. Surveillance will also serve to inform future vaccine development and revisions to national vaccine recommendations.
Reported by
HH Wrigley, MPH and S Petit, MPH, Epidemiology and Emerging Infections Program, Connecticut Department of Public Health.
Acknowledgments
C Marquez, A Hickey, MPH, D Wurm, MPH, Epidemiology and Emerging Infections Program; D Santoro, State Public Health Laboratory, Connecticut Department of Public Health.
References
1.CDC. 2020. Manual for the Surveillance of Vaccine-Preventable Diseases Chapter 11: Pneumococcal. https://www.cdc.gov/vaccines/pubs/surv-manual/chpt11-pneumo.html#f27.
2.CDC. 2021. Active Bacterial Core Surveillance Report, Emerging Infections Program Network, Streptococcus pneumoniae, 2020. https://www.cdc.gov/abcs/downloads/SPN_Surveillance_Report_2020.pdf.
3.Prasad N, Rhodes J, et. al. Changes in the Incidence of Invasive Bacterial Disease During the COVID-19 Pandemic in the United States, 2014-2020. J Infect Dis. 2023 Apr 12;227(7):907-916.
4.CDC. Vaccination Coverage by Age 24 Months Among Children Born in 2018 and 2019 — National Immunization Survey–Child, United States, 2019–2021. MMWR 2023, 72(2):33-38.
5.CDC. 2021. Pneumococcal vaccination coverage among adults 65 years of age or older, 2008-2021. https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/data-reports/general-population/index.html.
6.CDC. 2021. Pneumococcal vaccination coverage among adults 65 years of age or older, 2008-2021. https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/data-reports/general-population/index.html.
This page last updated 057/17/2023