September 2023 Page 2
Connecticut Epidemiologist Newsletter • September 2023 • Volume 43, No 6
The Impact of the COVID-19 Pandemic on Invasive Group A Streptococcus Incidence in Connecticut
Group A Streptococcus (GAS) bacteria can cause a range of illnesses from mild infections like strep throat and impetigo to more severe or life-threatening diseases including sepsis, cellulitis, necrotizing fasciitis, and streptococcal toxic shock syndrome. Severe manifestations of GAS typically result when disease is invasive (iGAS) and can lead to significant morbidity and mortality (1). The Center for Disease Control and Prevention (CDC) estimates that between 14,000 to 25,000 iGAS cases and 1,500 to 2,300 iGAS-associated deaths occur each year in the United States (2).
Incidence of iGAS increases with age. Individuals ≥65 years of age are at highest risk of severe disease with 14% dying following an iGAS infection. Long-term care facility (LTCF) residents are at even higher risk and are 1.5 times more likely to die following an iGAS infection than similarly aged adults living in the community (3). Other risk factors include injection drug use, wounds/skin disease, and chronic medical conditions such as diabetes, cancer, immunosuppression, and chronic kidney, cardiac, or respiratory disease (4).
During the first two years of the COVID-19 pandemic, iGAS incidence in the United States decreased by about 25% in all age groups with incidence in children at historic lows [1]. This was followed by an increase in pediatric iGAS in the fall of 2022 that prompted a CDC Health Advisory. Preliminary national 2022 data indicated that iGAS monthly incidence in children increased between September and November, earlier than the typical winter peak, concurrent with an increase in viral respiratory disease (4).
The Connecticut Department of Public Health (CT DPH) identifies iGAS cases (people with GAS identified in a normally sterile body site) through statewide active surveillance conducted by the Active Bacterial Core Surveillance project [5]. Given recent national fluctuations in iGAS incidence, this article examines annual incidence (per 100,000) trends among CT residents overall and by age group during the pandemic (2020–2022) compared to the average pre-pandemic (2013–2019) annual incidence. Seasonal trends were examined by comparing recent quarterly incidence (2022–June 2023) to the average pre-pandemic quarterly incidence overall and by age group.
In January 2013–June 2023, 1,555 iGAS cases were identified. During the initial two years of the pandemic, annual incidence decreased by 49% (95%CI: 28–68%) compared to the pre-pandemic average (4.1 per 100,000 annual average in 2013–2019 to 2.1 in 2021) followed by a resurgence in 2022 to 4.0. [Figure 1] This same pattern was seen in all adult age groups with the largest resurgence in 2022 among those 40–64 years of age who had a 211% (95%CI: 123–295%) increase (1.8 per 100,000 in 2021 to 5.6 in 2022). While annual incidence decreased during the initial two years of the pandemic among those <18 years of age, this age group did not experience a resurgence in 2022 like older age groups did. [Figure 2]

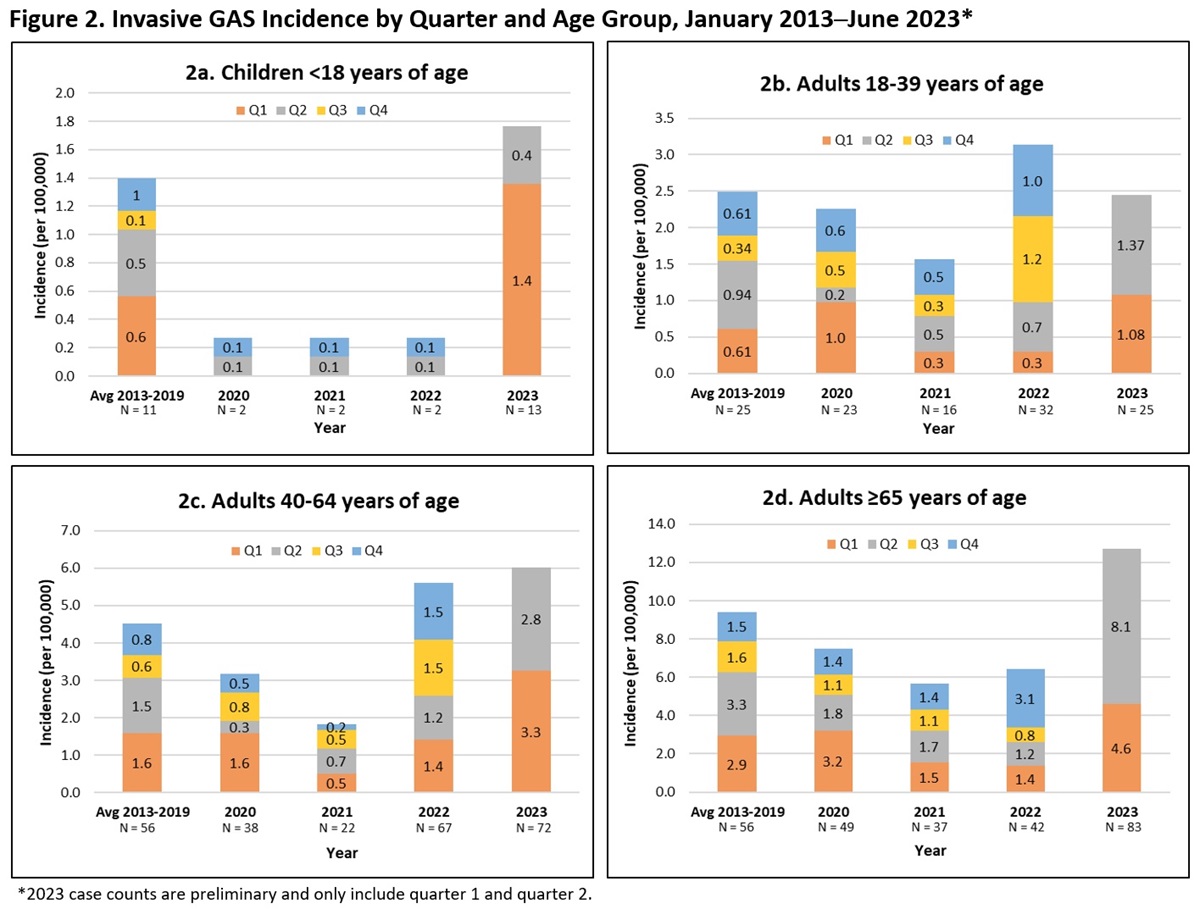
Overall incidence in the 4th quarter of 2022 was 75% (95%CI: 16–135%) higher than the pre-pandemic 4th quarter average (0.8 per 100,000 vs. 1.4) and was similar to rates typically seen in the 1st and 2nd quarters pre-pandemic. Increases continued into the 1st and 2nd quarters of 2023 when quarterly rates were 92% (95%CI: 42–140%) and 107% (95%CI: 54–151%) higher than corresponding quarter pre-pandemic averages (1.3 to 2.5 per 100,000 and 1.4 to 2.9 respectively). [Figure 1] This same pattern was seen among all adult age groups with the largest increases seen in those 40–64 years of age during the 1st quarter of 2023 (106%; 95%CI: 25–180%) and in those ≥65 years of age during the 2nd quarter of 2023 (138%; 95%CI: 59–218) (1.6 to 3.3 per 100,000 and 3.4 to 8.1 respectively). Among those <18 years of age, quarterly incidence remained lower than pre-pandemic averages until the 1st quarter of 2023 when it increased 180% (95%CI: -31–362%; 0.5 to 1.4 per 100,000) but then returned to average in the 2nd quarter of 2023. [Figure 2]
Discussion
In Connecticut, iGAS incidence in both children and adults decreased at the onset of the COVID-19 pandemic in 2020. This is consistent with trends seen in other states and has been attributed to COVID-19 related non-pharmaceutical interventions (1). Incidence of iGAS remained lower than average until a resurgence in late 2022 in adults and in early 2023 in children. Incidence during just the first half of 2023 was similar to or higher than the pre-pandemic average yearly incidence both overall and in each age group. Increases were highest among those ≥65 years of age. This is concerning as risk of severe disease and death increases with age. Despite increases in pediatric iGAS in the fall of 2022 in other areas of the county (4), Connecticut did not see an increase in pediatric disease until the 1st quarter of 2023. However, this increase was not sustained into the 2nd quarter of 2023 as it was for adult age groups. This is encouraging as it might signal a potential future decline to average incidence levels for older age groups in the latter half of 2023.
Since there is no vaccine available for GAS, early recognition and treatment are essential to reduce disease burden. Providers should educate patients on signs and symptoms of iGAS and offer recommended vaccinations for viral infections that might proceed or occur concurrently with iGAS (e.g., influenza and varicella). Additionally, providers should consider iGAS infection during severe illnesses and obtain cultures for suspected infection, including blood, wound, and pleural fluid as indicated. The CT DPH should be notified of potential clusters that are recognized especially in congregate settings. Residents of LTCFs are at particularly high risk and facility outbreaks can occur. CDC recently published a decision tool to guide LTCF personnel and public health officials in investigations of GAS infections in LTCFs (3). Prompt identification of iGAS cases in LTCFs is essential to allow for early intervention and implementation of the recommended control measures.
Continued iGAS surveillance is needed to assess whether changes in seasonal and age group incidence during the pandemic persist. Surveillance also allows for identification of clusters that might warrant public health intervention.
Reported by
A Hickey, MPH, S Petit, MPH, CT Department of Public Health Active Bacterial Core Surveillance Project
Acknowledgements
H H Wrigley, MPH, D Wurm, MPH, C Marquez
References
1. CDC. (2023, February 2). Increase in Invasive Group A Strep Infections, 2022–2023. Retrieved from https://www.cdc.gov/groupastrep/igas-infections-investigation.html
2. CDC. (2022, June 27). Surveillance. Retrieved from https://www.cdc.gov/groupastrep/surveillance.html
3. CDC. (2022, June 27). Group A Strep in Long-term Care Facilities: Identifying and Managing Outbreaks. Retrieved from https://www.cdc.gov/groupastrep/outbreaks/ltcf/index.html
4. CDC Health Alert Network (HAN). (2022, December 22). Increase in Pediatric Invasive Group A Streptococcal Infections. CDCHAN-00484. Retrieved from https://emergency.cdc.gov/han/2022/han00484.asp
5. Connecticut Department of Public Health. (2023, January). Changes to the List of Reportable Diseases, Emergency Illnesses and Health Conditions, and the List of Reportable Laboratory Findings. Connecticut Epidemiologist Newsletter, 43(1), 2. Retrieved from https://portal.ct.gov/DPH/Epidemiology-and-Emerging-Infections/The-Connecticut-Epidemiologist-Newsletter
This page last updated 10/05/2023