CFRP Annual Report Oct. 1, 2000 - Sept. 30, 2001
CHILD FATALITY REVIEW PANEL ANNUAL REPORT 2001
PANEL MEMBERS
Jeanne Milstein
Child Advocate
H.
Chief Medical Examiner
Regional Administrator
Department of Children and Families
Jane Norgren
Executive Director,
Honorable Arthur Spada
Commissioner of Public Safety
Pediatrician
Staff
Faith Vos Winkel
Assistant Program Director
MISSION
The Child Fatality Review Panel reviews child fatalities so that we may learn how to prevent future deaths. The panel’s purpose is to save lives by learning from lives lost. Thorough review of infant and child deaths is the key to recognizing what types of death are preventable and taking steps to protect children from harm.
DEVELOPMENTS
During the past two years, the Governor, legislature and the panel have taken steps that will greatly improve the panel’s ability to fulfill its mission. The Governor and legislature authorized the panel to review all unexpected or unexplained deaths. Until
In September 2000, the panel improved the review process with the development of a fatality review data form that will capture detailed information about every unexplained or unexpected death. The data form will be incorporated into a relational database to better manage and analyze the information gathered. By tracking and studying this data, we can recognize patterns of risk and recommend ways to save lives.
“Lack of adequate investigations of infant
and child deaths allow flawed
systems to continue and are an impediment to
preventing illness,
injury, and the death of other children at risk.”
American
Overview
This annual report covers the period from
from
174 child fatalities were reported to the
child fatality review panel
Automobile accidents remained a significant cause of death in this age group. Sixteen youngsters in the group (24%) died in automobile accidents. Of those 16 youth who died in motor vehicle accidents 13 were 16 & 17 years olds.
Complex medical conditions, both congenital and acquired, accounted for the largest number of fatalities, a total of 60 (34%). Sudden Infant Death Syndrome (SIDS) accounted for 24 deaths (14%). Motor vehicle related accidents were the leading cause of reported fatalities in the last report; it also remains the leading cause of accidental death for children for this reporting period, with 30 (17%).
A total of 94 (54%) children ages six and younger made up the single largest group of child fatalities. Complex medical conditions, congenital and acquired, accounted for 36 of those deaths (20%), followed closely by SIDS. In the age group between 7 through 17 years, a total of 80 (46%) children died.
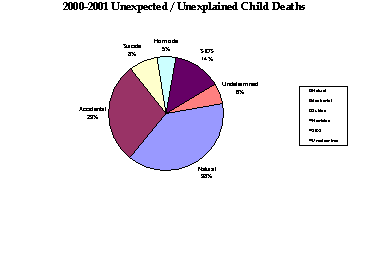
The manner of death was classifed as:
§ Natural: 91 children (52%)
Including 24 SIDS
§ Accidental: 50 children (29%)
§ Suicide: 14 (8%)
§ Homicide: 9 children (5%)
§ Undetermined: 10 children (6%)
GOALS
Now that the child fatality review data form is in use, the panel will develop a database to record the information. By studying these details, we will identify trends and patterns of risk in order to prevent future deaths.
In the case of SIDS, for example, data will be collected about where the baby was sleeping, how the baby was positioned for sleep, how the baby was positioned at the time of death, and other details that may help explain infants who died of SIDS. Currently, the Office of the Chief Medical Examiner maintains a SIDS data collection protocol that is quite comprehensive. Law enforcement officials complete this data collection form at the scene. This information will be coordinated with the panel and integrated into the CFRP database.
In the case of a motor vehicle accident, the panel will record whether the victim was restrained in a car seat or by a seat belt, the type of vehicle, the age of the driver, where the victim was positioned in the vehicle, the road condition, whether airbags deployed, the time of day, how many people were in the vehicle and other details that will describe factors that contribute to motor vehicle deaths.
Hospitals, police and other entities report all unexplained, unexpected or unattended (outside of a hospital) deaths of children to the Office of the Chief Medical Examiner (OCME). All of those deaths reported to the OCME are in turn reported to the OCA and the CFRP. When the body of a child is cremated, the death is reported to the OCME, regardless of the nature of the death. These are also reported to the OCA and the CFRP. Under
Many childhood deaths are preventable, but only if we understand how and why children die. More detailed information and complete reporting will help the panel to develop a greater understanding of child fatalities in order to develop appropriate prevention strategies.
“Injuries are the leading killer of our children. . .
We call them accidents,
but they’re not, because they can
be predicted and prevented.
It doesn’t cost a lot or take much time, either.
Just the attention and effort of parents and other caregivers.”
A program of Connecticut Children’s
Child Fatality Data
The remainder of this report focuses on the child fatalities that were reported to the Office of the Chief Medical Examiner and reviewed by the panel between
Natural Deaths
Sixty-seven children (38% of total fatalities) died of natural causes. Natural causes included asthma, acute illness, seizures, complications related to premature birth and complex medical conditions, both congenital and acquired.
SUDDEN INFANT DEATH SYNDROME
Twenty-four babies died of SIDS, which is defined as “the sudden death of a healthy infant less than one year of age that remains unexplained after the performance of a complete post mortem investigation, including an autopsy, an examination of the scene of death, and review of the case history.[1]”
Most of the infants who died of SIDS were between two and four months of age. Ten infants died of SIDS during their second month of life. Seven babies who died of SIDS were in their third and four months. The infants ranged in age from four weeks to seven months.
Preventable deaths
Seventy-three children (42% of total fatalities) died of preventable causes, including motor vehicle related accidents, asphyxiation from a venetian blind cord, being buried in the sand, playing with a dog leash, and other accidental injures such as falling, choking, and drowning. Other deaths considered preventable by the panel were homicide and suicide.
MOTOR VEHICLE ACCIDENTS
Thirty children died in motor vehicle related accidents. This is the leading cause of accidental death among
DROWNING
Eleven children died by drowning during the year. Five of those were six years old or younger. Five of these victims drowned in natural bodies of water, while most of the others succumbed in tubs or pools. One child drowned in a boating accident.
SUICIDE
Suicide accounted for 14 (8%) of the 174 deaths. This is an especially significant problem among adolescents. Teen males committed suicide at a much greater rate than females. All but one of the suicide deaths were male children. Seventy-nine percent of those who took their own lives were white males. The method of choice for the vast majority (11) of those young people who took their own lives was hanging. The three additional children used firearms.
HOMICIDE
There were nine homicides during this reporting period. The four children under age six that were killed were done so by a family member or a known care giver. The five young men killed in the 16-17 age groups were victims of gunshot wound.
“If a disease were killing our children in the proportions that accidents are, people would be outraged and demand that this killer be stopped.”
National Safe Kids Campaign
Special Investigations
There are several levels of investigation of child fatalities by the review panel. Some of the fatalities are noted and tracked to characteristic and trends. Others may be noted and any resulting investigations by other public agencies such as police or child protective services are monitored for outcomes and findings. The highest level of investigation by the CFRP results in a published public report of the death. These reports are the result of in-depth investigation of all persons, agencies, and systems involved in that child’s life leading up to that child’s death. The purpose of these investigations is to identify whether there are inadequacies in the systems meant to protect the child and to develop recommendations to improve child protection and welfare practices.
In March 2001, a joint investigation by the Office of the Child Advocate and the Child Fatality Review Panel was released regarding the death of a child named
Conclusion
A review of child deaths between October 2000 and September 2001 revealed a disturbing and ongoing trend of increasing numbers of preventable deaths.
The largest category of deaths, were among children with complex medical conditions, suggests an increase in survival rates among children with congenital conditions who may not have survived in the past. Mortality is actually down in early childhood among infants at risk. However, what has occurred is a new and growing population of children at high risk of morbidity and thus high risk of childhood deaths. As the CFRP continues to monitor and analyze the deaths of these children, they also support the work the OCA has focused on children with special health care needs. OCA is working to identify system improvements to assure better care of children with special health care needs and longer, healthier lives.
The growing suicide rate among children in
Finally, accidents, including drowning, and especially motor vehicle accidents, continue to be leading causes of death among children that are wholly preventable.
As a result of the CFRP’s findings, initiatives have been undertaken to better educate children and the community, families, and schools about preventing accidents. The Child Fatality Review Panel has made a great deal of progress in the past year towards establishing a system to quantify and describe the unexpected and unexplained deaths of children in the state. Improved data collection and better communication of relevant data with the Chief Medical Examiner will assure accurate accounts of child deaths. Consequently, analysis of causes of deaths, trends in deaths, and over all system inadequacies will be improved. Effective analysis will allow identification of opportunities to improve systems that keep children well and safe.
Child fatality reviews are important because they “have the potential to accelerate progress in the understanding of SIDS, reduce the number of fatal cases of child abuse and neglect that are missed, increase the awareness of familial genetic diseases, focus attention on public health threats, and detect and remediate inadequate medical care. (
cfrp accomplishments year 2002-2001
q Established a full-time position with the support of the Governor’s Office and OPM for a staff person to devote full attention to the work of the CFRP and other OCA activities regarding child fatalities.
q Implemented a data collection system to capture relevant information regarding trends in child fatalities.
q Developed a blueprint for a comprehensive database system.
q Initiated outreach to the larger child welfare system to begin to develop a framework for collaborative prevention initiatives.
q Distributed over 200 copies of the CFRP annual report and investigative fatality reports.
q Participated as a member of the Interagency Suicide Prevention Network.
q Participated as a member of the DCF Advisory Committee on Youth Suicide.
q Participated as a member for the fatality review of domestic violence issues.
q All child fatality investigations are posted on the web at www.oca.state.ct.us
Focus Areas
q Increase the membership of the panel to include a representative from the Department of Public Health, Connecticut Coalition Against Domestic Violence, and a representative from the disability community.
q Develop a process to ensure that family members who want to speak with the panel have an opportunity to do so.
q Continue to forge alliances with other agencies and entities with a focus on prevention initiatives.
q Publish reports as necessary to educate the public on policy issues.
|
|
Under One Year |
One thru Three |
Four thru Six |
Seven thru Ten |
Eleven thru Fifteen |
Sixteen thru Seventeen |
Total |
accidental death |
|
|
|
|
|
|
|
|
Automobile Accident |
2 |
3 |
|
1 |
3 |
13 |
22 |
|
Motor vehicle accidents Involving pedestrians, roller blades, bicycles, etc. |
|
3 |
|
|
4 |
1 |
8 |
|
Drowning |
|
3 |
2 |
|
5 |
1 |
11 |
|
Fire/Burns |
|
|
|
|
|
|
0 |
|
Accidental Injury |
1 |
3 |
|
2 |
2 |
1 |
9 |
homicide
|
|
2 |
2 |
|
|
5 |
9 |
Suicide
|
|
|
|
|
3 |
11 |
14 |
natural
|
|
|
|
|
|
|
|
|
Complex Medical Conditions Acquired & Congenital |
23 |
6 |
7 |
9 |
8 |
7 |
60 |
|
Acute Illness |
|
3 |
|
1 |
2 |
|
6 |
|
Asthma |
|
|
1 |
|
|
|
1 |
|
SIDS |
24 |
|
|
|
|
|
24 |
Undetermined
|
6 |
2 |
1 |
1 |
|
|
10 |
RELEVANT STATUTES
Connecticut General Statutes sec. 46a-131 (b) and (c):
STATUTES RELATING TO THE OFFICE OF THE CHILD ADVOCATE
(INCLUDING 2001 AMENDMENTS)[*]
Sec. 46a-13k. Office of the Child Advocate established. (a) There is established an office of the Child Advocate. The Governor, with the approval of the General Assembly, shall appoint a person with knowledge of the child welfare system and the legal system to fill the Office of the Child Advocate. Such person shall be qualified by training and experience to perform the duties of the office as set forth in section 46a-13l. The appointment shall be made from a list of at least three persons prepared and submitted by the advisory committee established pursuant to section 46a-13q. Upon any vacancy in the position of Child Advocate, the advisory committee shall meet to consider and interview successor candidates and shall submit to the Governor a list of no less than five and no more than seven of the most outstanding candidates, on or before sixty days of said vacancy. Such list shall rank the candidates in the order of committee preference. Upon receipt of the list of candidates from the advisory committee, the Governor shall designate a candidate for Child Advocate from among the choices within eight weeks of receipt of such list. If at any time any of the candidates withdraw from consideration prior to confirmation by the General Assembly, the designation shall be made from the remaining candidates on the list submitted to the Governor. If a candidate has not been designated by the Governor within the eight-week time period, the candidate ranked first shall receive the designation and be referred to the General Assembly for confirmation. If the General Assembly is not in session, the designated candidate shall serve as acting Child Advocate, and be entitled to the compensation, privileges and powers of the Child Advocate until the General Assembly meets to take action on said appointment. The person appointed Child Advocate shall serve for a term of four years and may be reappointed or shall continue to hold office until such person’s successor is appointed and qualified. Upon any vacancy in the position of Child Advocate and until such time as a candidate has been confirmed by the General Assembly or, if the General Assembly is not in session, has been designated by the Governor, the Associate Child Advocate shall serve as the acting Child Advocate and be entitled to the compensation, privileges and powers of the Child Advocate.
(b) The Office of the Child Advocate shall be in the Freedom of Information Commission for administrative purposes only.
(c) Notwithstanding any other provision of the general statutes, the Child Advocate shall act independently of any state department in the performance of his duties.
(d) The Child Advocate may, within available funds, appoint such staff as may be deemed necessary provided, for the fiscal years ending
(e) The General Assembly shall annually appropriate such sums as necessary for the payment of the salaries of the staff and for the payment of office expenses and other actual expenses incurred by the Child Advocate in the performance of his duties. Any legal or court fees obtained by the state in actions brought by the Child Advocate shall be deposited in the General Fund.
(f) The Child Advocate shall annually submit to the Governor and the General Assembly a detailed report analyzing the work of the Office of the Child Advocate.
(
History:
See Sec. 4-38f for definition of “administrative purposes only”.
Sec. 46a-13l. Child Advocate’s duties. Child fatality review panel. Reports to the Governor and the General Assembly. Investigations. (a) The Child Advocate shall:
(1) Evaluate the delivery of services to children by state agencies and those entities that provide services to children through funds provided by the state;
(2) Review periodically the procedures established by any state agency providing services to children to carry out the provisions of sections 46a-13k to 46a-13q, inclusive, with a view toward the rights of the children and recommend revisions to such procedures;
(3) Review complaints of persons concerning the actions of any state or municipal agency providing services to children and of any entity that provides services to children through funds provided by the state, make appropriate referrals and investigate those where the Child Advocate determines that a child or family may be in need of assistance from the Child Advocate or that a systemic issue in the state’s provision of services to children is raised by the complaint;
(4) Pursuant to an investigation, provide assistance to a child or family who the Child Advocate determines is in need of such assistance including, but not limited to, advocating with an agency, provider or others on behalf of the best interests of the child;
(5) Periodically review the facilities and procedures of any and all institutions or residences, public or private, where a juvenile has been placed by any agency or department;
(6) Recommend changes in state policies concerning children including changes in the system of providing juvenile justice, child care, foster care and treatment;
(7) Take all possible action including, but not limited to, conducting programs of public education, undertaking legislative advocacy and making proposals for systemic reform and formal legal action, in order to secure and ensure the legal, civil and special rights of children who reside in this state;
(8) Provide training and technical assistance to attorneys representing children and guardians ad litem appointed by the Superior Court;
(9) Periodically review the number of special needs children in any foster care or permanent care facility and recommend changes in the policies and procedures for the placement of such children;
(10) Serve or designate a person to serve as a member of the child fatality review panel established in subsection (b) of this section; and
(11) Take appropriate steps to advise the public of the services of the Office of the Child Advocate, the purpose of the office and procedures to contact the office.
(b) There is established a child fatality review panel composed of seven permanent members as follows: A pediatrician, appointed by the Governor; a representative of law enforcement, appointed by the president pro temporare of the Senate; the Child Advocate, or a designee; a public child welfare practitioner, appointed by the minority leader of the Senate; a representative of a community service group appointed by the speaker of the House of Representatives; a medical examiner, appointed by the minority leader of the House of Representatives; and the Chief State’s Attorney, or a designee. A majority of the panel may select not more than two additional temporary members with particular expertise or interest to serve on the review of a specific fatality. Such temporary members shall have the same duties and powers as the permanent members of the panel. The chairperson shall be elected from among the panel’s permanent members. The panel shall, to the greatest extent possible, reflect the ethnic, cultural and geographic diversity of the state.
(c) The panel shall review the circumstances of the death of a child placed in out-of-home care or whose death was due to unexpected or unexplained causes to facilitate development of prevention strategies to address identified trends and patterns of risk and to improve coordination of services for children and families in the state. Members of the panel shall not be compensated for their services, but may be reimbursed for necessary expenses incurred in the performance of their duties.
(d) On or before
(e) Upon request of two-thirds of the members of the panel and within available appropriations, the Governor, the General Assembly or at the Child Advocate’s discretion, the Child Advocate shall conduct an in-depth investigation and review and issue a report with recommendations on the death or critical incident of a child. The report shall be submitted to the Governor, the General Assembly and the commissioner of any state agency cited in the report and shall be made available to the general public.
(f) The Chief Medical Examiner shall provide timely notice to the Child Advocate and to the chairperson of the child fatality review panel of the death of any child that is to be investigated pursuant to section 19a-406.
(g) Any agency having responsibility for the custody or care of children shall provide timely notice to the Child Advocate and the chairperson of the child fatality review panel of the death of a child or a critical incident involving a child in its custody or care.
(
History:
Sec. 46a-13m. Access to information. (a) Notwithstanding any provision of the general statutes concerning the confidentiality of records and information, the Child Advocate shall have access to, including the right to inspect and copy, any records necessary to carry out the responsibilities of the Child Advocate as provided in subsection (a) of section 46a-13l. If the Child Advocate is denied access to any records necessary to carry out said responsibilities, he may issue a subpoena for the production of such records as provided in subsection (c) of this section.
(b) In the performance of this responsibilities under subsection (a) of section 46a-13l the Child Advocate may communicate privately with any child or person who has received, is receiving or should have received services from the state. Such communications shall be confidential and not be subject to disclosure except as provided in subsection (a) of section 46a-13n.
(c) The Child Advocate may issue subpoenas to compel the attendance and testimony of witnesses or the production of books, papers and other documents and to administer oaths to witnesses in any matter under his investigation. If any person to whom such subpoena is issued fails to appear or, having appeared, refuses to give testimony or fails to produce the evidence required, the Child Advocate may apply to the superior court for the judicial district of Hartford which shall have jurisdiction to order such person to appear and give testimony or produce such evidence, as the case may be.
(d) The Child Advocate may apply for and accept grants, gifts and bequests of funds, from other states, federal and interstate agencies and independent authorities and private firms, individuals and foundations, for the purpose of carrying out his responsibilities. There is established within the General Fund a child advocate account which shall be a separate nonlapsing account. Any funds received under this subsection shall, upon deposit in the General Fund, be credited to said account and may be used by the Child Advocate in the performance of his duties.
(P.A. 88-230, S. 10, 12; P.A. 90-98, S. 1, 2; P.A. 93-142, S. 7, 8; P.A. 95-220, S. 4-6; P.A. 95-242, S. 8; P.A. 97-319, S. 4.)
History: P.A. 97-319 entirely replaced former section with new provisions re access to information (Revisor’s note: P.A. 88-230, 90-98, 93-142 and 95-220 authorized substitution of “judicial district of Hartford” for “judicial district of Hartford-New Britain” in 1998 public and special acts, effective September 1, 1998).
(b) No state or municipal agency shall discharge, or in any manner discriminate or retaliate against, any employee who in good faith makes a complaint to the Child Advocate or cooperates with the Office of the Child Advocate in an investigation.
(
History: P.A. 96-268 substituted Office of the Child Advocate for Child Advocate’s Office, effective July 1, 1996; P.A. 97-319 entirely replaced former section with new provisions re confidentiality; June Sp. Sess. P.A. 99-2 amended Subsec. (a)(2) by deleting “provided in no event shall the name, address or other personally identifiable information of a person be disclosed without the consent of such person” and made technical changes.
(b) Any judgment for compensation or order for settlement of the claim for compensation entered by the court pursuant to the provisions of subsection (a) of this section shall be considered as the estate of the child for whose benefit the judgment or order is entered, to be held by the Office of the Child Advocate as guardian of such compensation, and shall be deposited into a trust account established by the office for the purposes of distributing such funds to such child in accordance with the plan adopted by the Family Division of the Superior Court.
(
History:
(
(b) Said advisory committee shall consist of one pediatrician, appointed by the majority leader of the House of Representatives; one public child welfare social worker, appointed by the minority leader of the House of Representatives; one psychologist, appointed by the Connecticut Psychological Association; one attorney, appointed by the Connecticut Bar Association; one judge of the Family Division of the Superior Court, appointed by the Chief Justice of the Supreme Court; one representative of private children’s agencies, appointed by the appointed by the president pro tempore of the Senate; and one representative of education, appointed by the minority leader of the Senate. Each member of the advisory committee shall serve a five-year term.
(c) Said advisory committee shall provide authorization to the Child Advocate for initiating a legal action against a state department in Superior Court.
(
[*]NOTE: This compilation of the statutes concerning the Office of the Child Advocate is unofficial and for the convenience of the public only. While every effort was made to attain complete accuracy herein, the reader is advised to consult the Connecticut General Statutes for the official codification of the law.